
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-068
PCI for LAD-M CTO From Auto-Collateral and RCA-CTO in One Patient
By Hsu Chung Lo
Presenter
Hsu chung Lo
Authors
Hsu Chung Lo1
Affiliation
Taichung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-068
CORONARY - Chronic Total Occlusion
PCI for LAD-M CTO From Auto-Collateral and RCA-CTO in One Patient
Hsu Chung Lo1
Taichung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
001729423E
Relevant Clinical History and Physical Exam
This is a 79-year-old male who had past medical history of hypertension and diabetes and hypertension under medication control. This time, he came to reginal hospital for help due to progressed left anterior chest tightness for 1 week. Non-ST elevation myocardial infarction was diagnosed there. First attempt of percutaneous coronary intervention was failed there. Therefore, he was transferred to our hospital for second opinion.
Relevant Test Results Prior to Catheterization
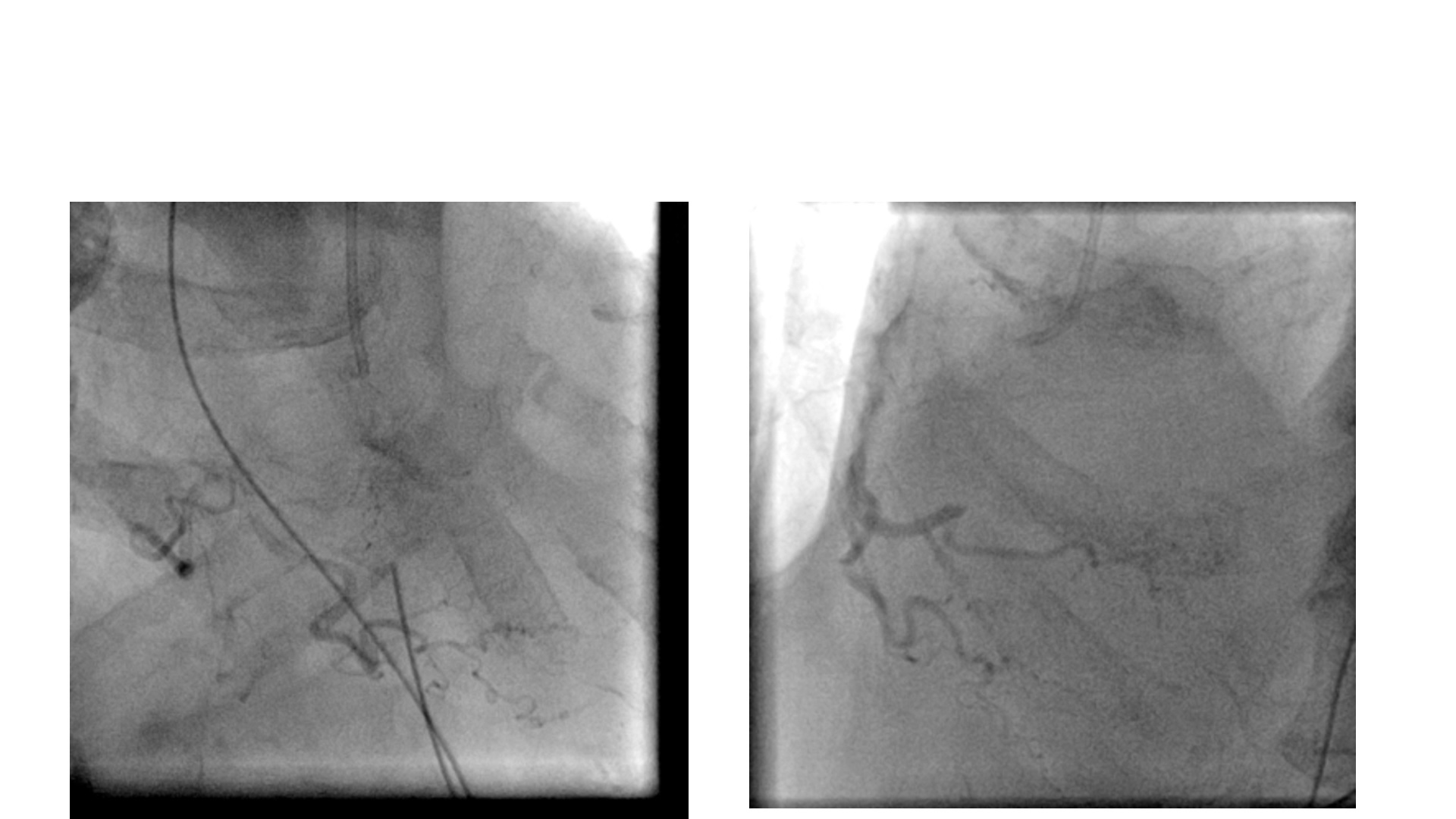
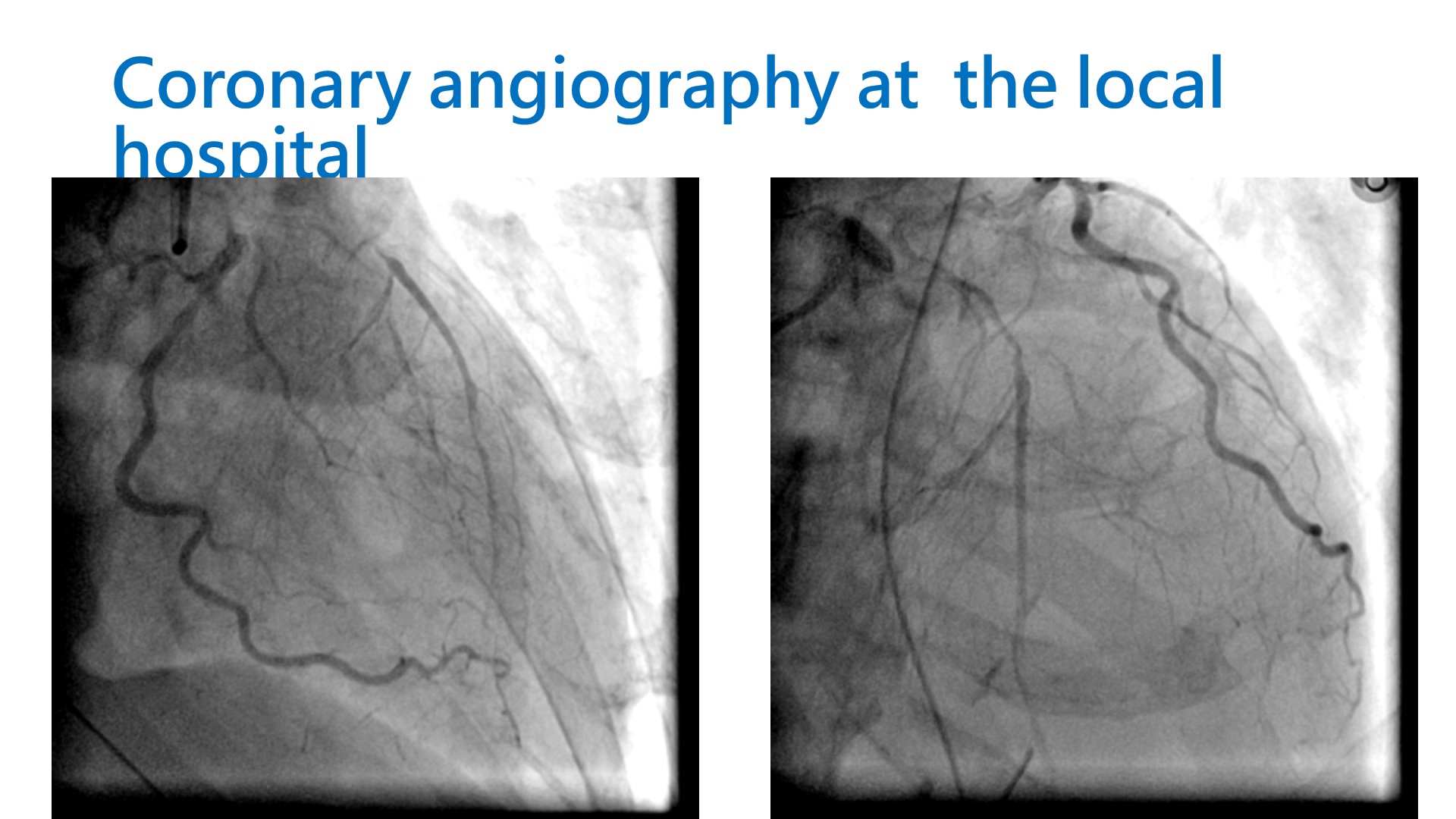
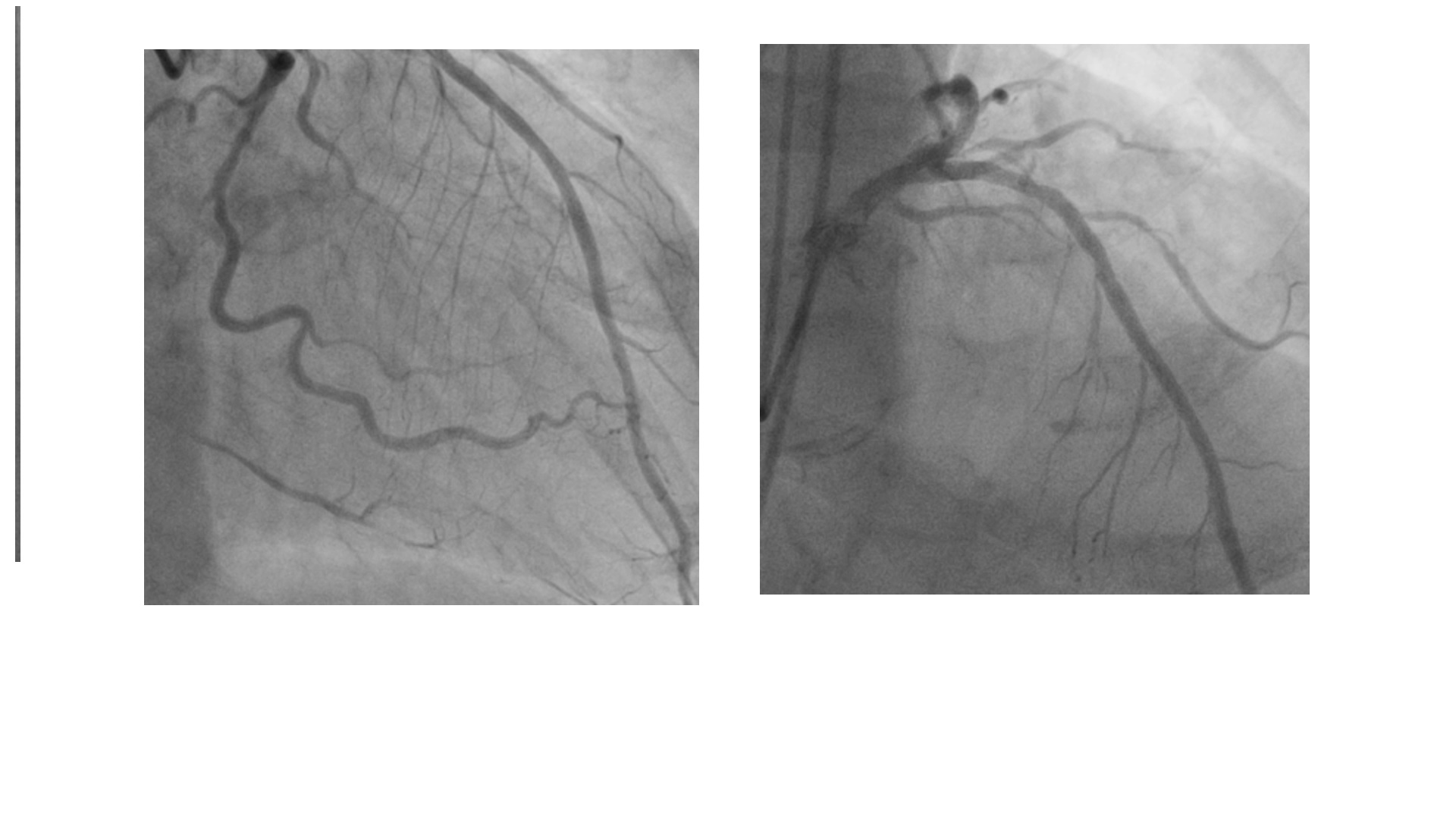
Relevant Catheterization Findings
Coronary angiography revealed chronic total occlusion of LAD and RCA. LCX proximal 80-90% stenosis.
Interventional Management
Procedural Step
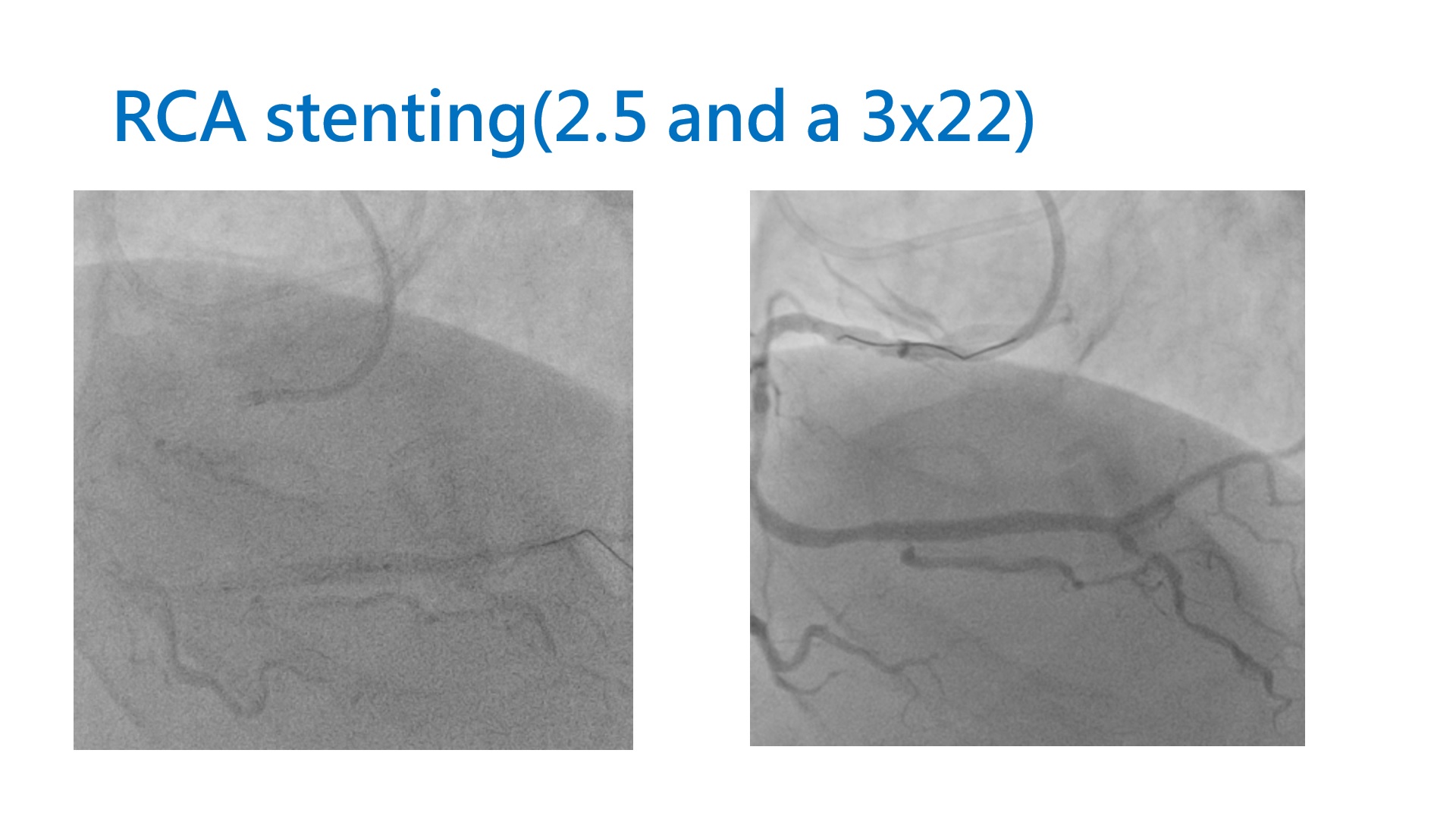
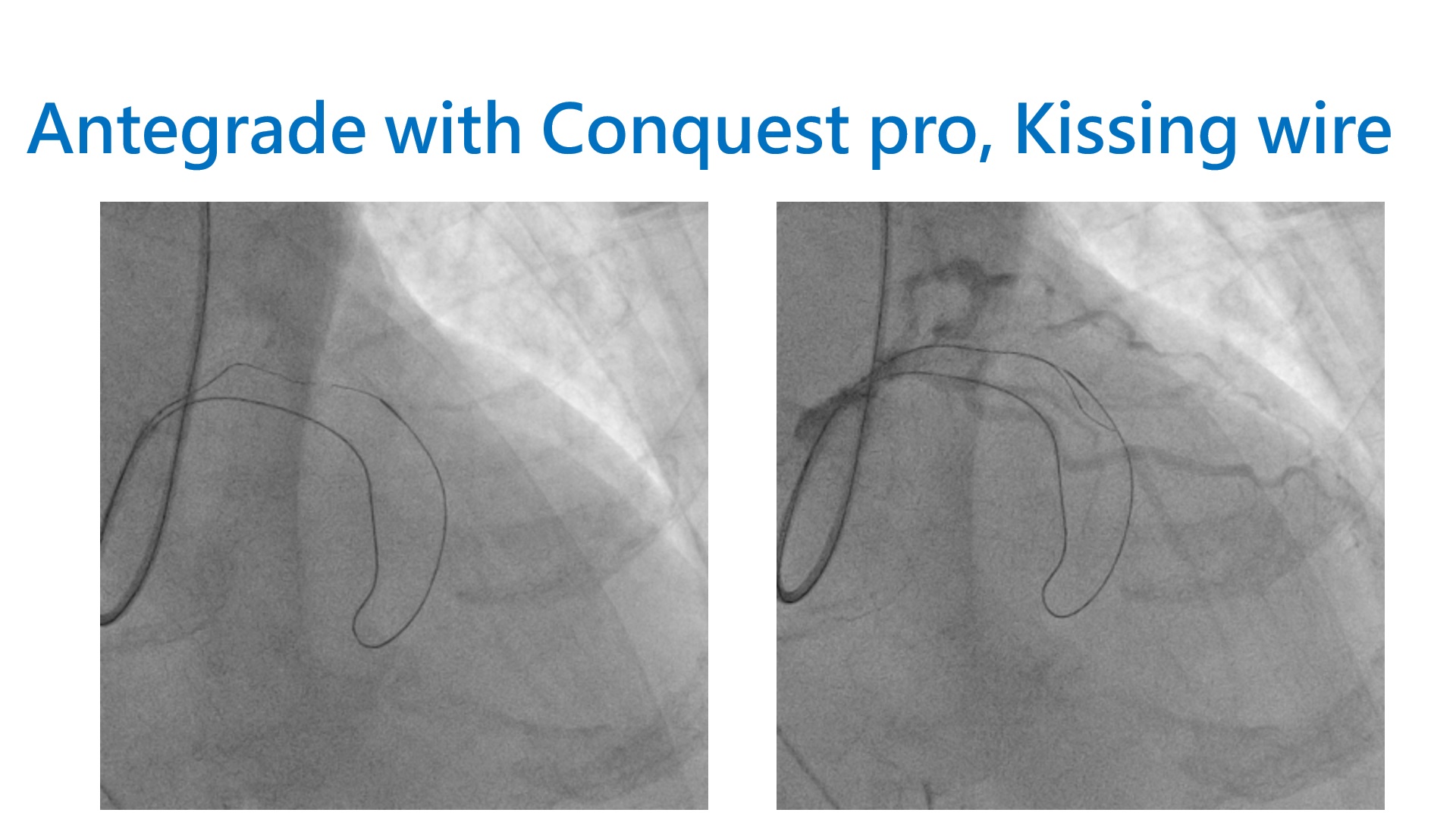
PCI for LAD was approached with XB 3.5x6F guide. Due to acute angulation, the first septal branch was very difficult to engage and could only be entered by keeping the guide coaxial with LM after advancing a Sion Blue to LCX. After the Mizuki was advanced to the body of first septal branch, the septal to septal collateral could be successfully wired with a Fielder XT-R, followed by advancement of the Mizuki to LAD proper. However, the distal CTO cap was very hard and failed to be crossed with either Fielder XT-A, UB 3, Gaia 2 or Conquest pro. Antegrade wiring then followed and the CTO body could be entered with a Conquest Pro and successful antegrade wiring was made with a Conquest Pro using kissing wire technique. The CTO was sequentially dilated with a 1.5x20mm and a 2.5x20mm BC. Due to LCX-os-P lesion, the LCX was wired with a Sion Blue. Distal LM to LCX-P was scaffolded with a 2.5x26mm Onyx. The LAD-P-M and LM-LAD-P were scaffolded with a 3x20mm Synergy and a 2.75x30mm Onyx. Then LCX was rewired with a Sion Blue, as aided by a Crusade, and the opening was dilated with a 2x20mm BC, inflated up to 16 bars. Final KBT was done using a 3x20mm BC in the LM-LAD-P and Lcx. The LM was further dilated with a 5x8mm NC BC. PCI for RCA was used SAL 1,5 X6F. The CTO segment could be successfully wired with an UB3, as supported by a Caravelle. The distal wire poistion confirmed by contralateral injection. RCA-PL could be loop wired with a Fielder FC. RCA-D-Pl and RCA-D were scaffolded with stents.
Case Summary
•Septalto septal collateral crossing is a viable option for retrograde PCI in selectedcases
•Sharperwire tip curve is needed in case of septal to septal collateral crossing due toacute angulations
•Kissingwire technique is a simple but invaluable skill in retrograde PCI practice