
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-023
A Forgotten Cause of ST Elevation Myocardial Infarction
By Ting Yuen Beh, Wei Liang Lee, Chee Kiang Teoh
Presenter
Ting Yuen Beh
Authors
Ting Yuen Beh1, Wei Liang Lee1, Chee Kiang Teoh1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-023
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
A Forgotten Cause of ST Elevation Myocardial Infarction
Ting Yuen Beh1, Wei Liang Lee1, Chee Kiang Teoh1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Mr. S
Relevant Clinical History and Physical Exam
65 years old Indian gentleman with no known medical illness, presented with acute central chest pain associated with dyspnoea. There was no gastrointestinal symptom and no diaphoresis. Clinical examination was unremarkable with BP 120/70, HR 88, SPO2 99% on room air. Lungs were clear and S1S2 heard with no murmur. No signs of pulmonary congestion. ECG showed ST elevation over inferior leads and he was diagnosed with acute inferior myocardial infarct Killip I.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
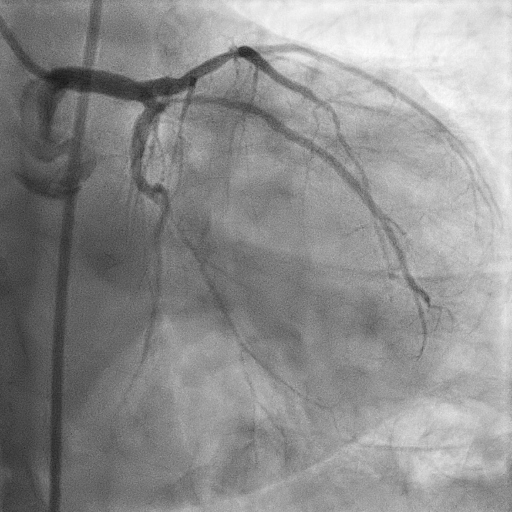
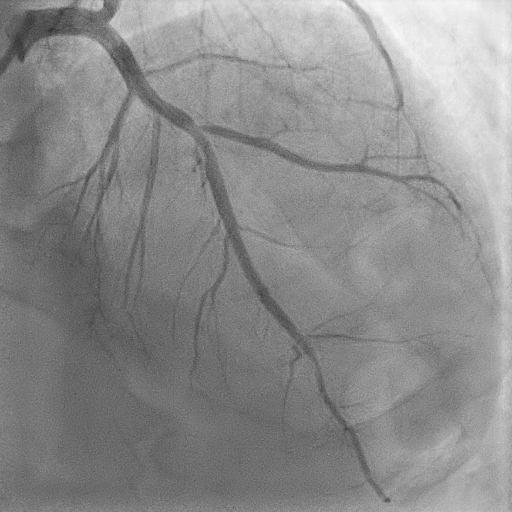
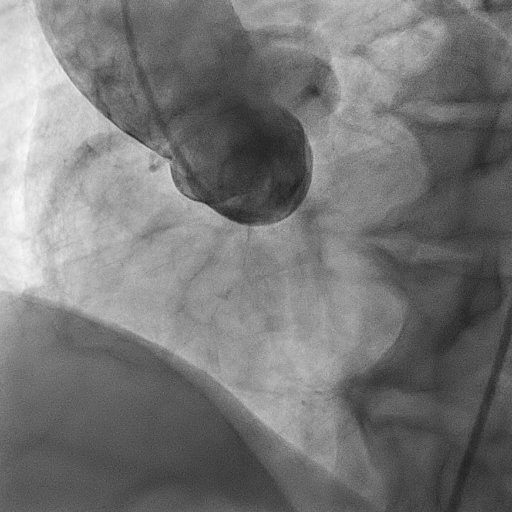
Coronary angiogram showedLeft main stem: normalLeft anterior descending artery: mild disease at mid segmentLeft circumflex artery: small; mild disease at obtuse marginal arteryRight coronary artery: anomalous RCA; unable to engage with JL, JR or Castillo 2 catheters. Aortogram done showed RCA likely originating from left cusp. Procedure abandoned as patient asymptomatic and ST elevation has resolved.
Interventional Management
Procedural Step
After the diagnostic shots to the left system, we tried multiple times to engage the RCA. However, we failed despite using JR, JL and Castillo catheters. Eventually we used aortogram which showed anomalous RCA, likely originating from the left cusp. As patient's chest pain had resolved during the attempted primary percutaneous coronary angiogram, we performed a 12lead ECG which showed resolution of ST elevation over inferior leads. Subsequently, procedure was abandoned. He was given dual antiplatete therapy and s/c fondaparinux, monitored closely in coronary care unit. Coronary CT angiography was performed to look for malignant anomalous RCA.
It showed mild disease in proximal segment of LAD and mild disease at proximal segment of OM. Anomalous origin of RCA malignant type. The proximal segment of RCA is in between aorta and main pulmonary artery with slit-like vessel shaped (malignant course). Subsequently, he was referred to cardiothoracic surgeon for coronary artery bypass surgery.

It showed mild disease in proximal segment of LAD and mild disease at proximal segment of OM. Anomalous origin of RCA malignant type. The proximal segment of RCA is in between aorta and main pulmonary artery with slit-like vessel shaped (malignant course). Subsequently, he was referred to cardiothoracic surgeon for coronary artery bypass surgery.
Case Summary
This case illustrates an atypical presentation of acute coronary syndrome (acute inferior myocardial infarction) which revealed anomalous course of RCA. In view of its malignant course, the patient is subjected to coronary artery bypass surgery. As we could not engage the RCA during coronary angiogram, one should suspect anomalous origin as a potential cause. Therefore, CCTA could assist us in determining whether it is a really an anomalous origin with benign or malignant course. The use of imaging is crucial in this scenario.