
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-040
Intravascular Lithotripsy in Left Main Coronary Artery
By Kuntal Bhattacharya, Debdatta Bhattacharyya, Ayan Kar, Koushik Dasgupta, Snehil Goswami
Presenter
Ayan Kar
Authors
Kuntal Bhattacharya1, Debdatta Bhattacharyya2, Ayan Kar1, Koushik Dasgupta1, Snehil Goswami3
Affiliation
NH-Rabindranath Tagore International Institute of Cardiac Sciences, India1, RN Tagore Hospital, India2, NH MMI Hospital, India3,
View Study Report
TCTAP C-040
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Intravascular Lithotripsy in Left Main Coronary Artery
Kuntal Bhattacharya1, Debdatta Bhattacharyya2, Ayan Kar1, Koushik Dasgupta1, Snehil Goswami3
NH-Rabindranath Tagore International Institute of Cardiac Sciences, India1, RN Tagore Hospital, India2, NH MMI Hospital, India3,
Clinical Information
Patient initials or Identifier Number
JR
Relevant Clinical History and Physical Exam
64 year chronic smoker presented with unstable angina despite maximal antianginal therapy and claudication pain after walking 150m.Underwent CAG which showed ostial left main + triple vessel disease.Prior to surgical work up found to have left subclavian stenosis , diseased LIMA , bilateral renal artery stenosis and bilateral peripheral arterial disease.Advised CABG.Surgical turndown for porcelain aorta and high surgical risk .advised HR PCI after institute heart team meet

Relevant Test Results Prior to Catheterization
Hb:16.4 ,creat 1.2mg/dl, hs tropI < 1.5ng/mlEcho no RWMA LVEF 64%bilateral minor carotid diseaseBilateral below-knee severe peripheral arterial disease

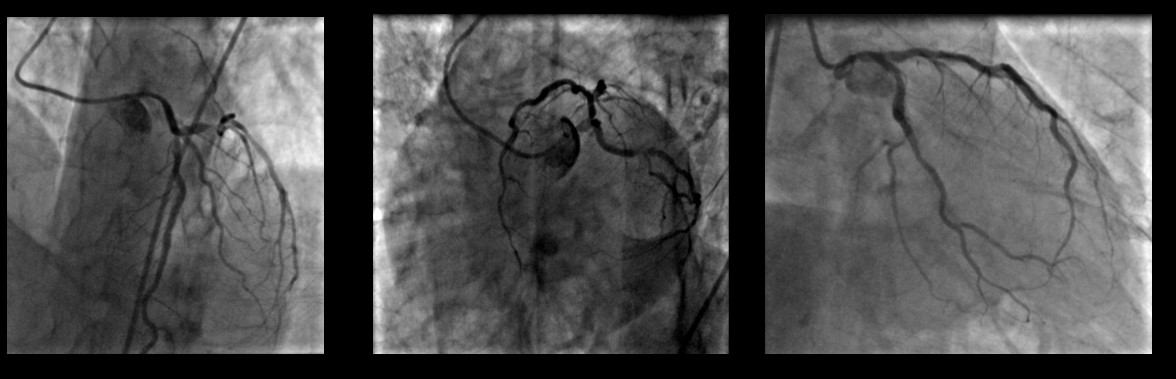
Relevant Catheterization Findings
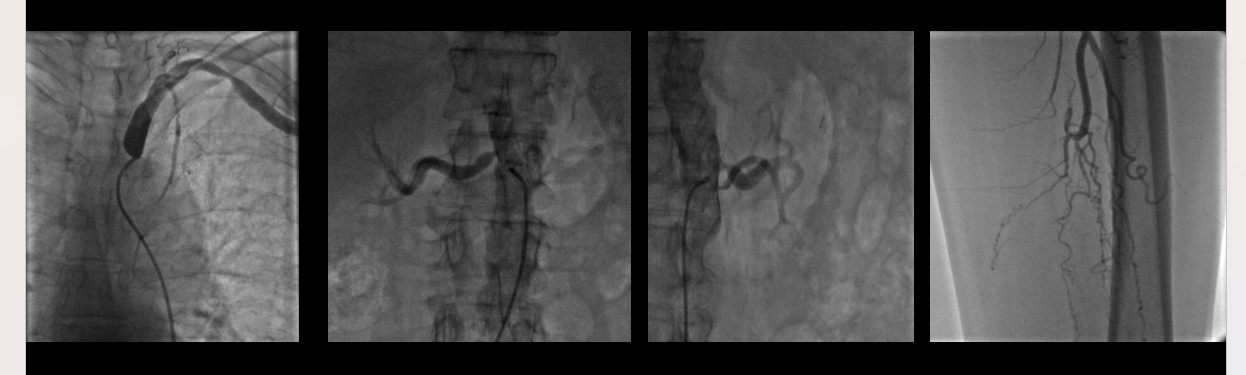
Ostial LMCA calcific disease with 70% stenosis mid LAd shows 70% stenosisLCX shows discrete 90% stenosis in the mid partRCA is tortuous with tight calcific long segment disease involving proximal and mid-RCA with 80% diameter stenosis. Distal PDA is occluded significant disease in the left common iliac ostiumleft subclavian stenosis with the tight disease in the ostial left vertebral artery, LIMA is diseasedbilateral significant renal artery stenosis
Interventional Management
Procedural Step
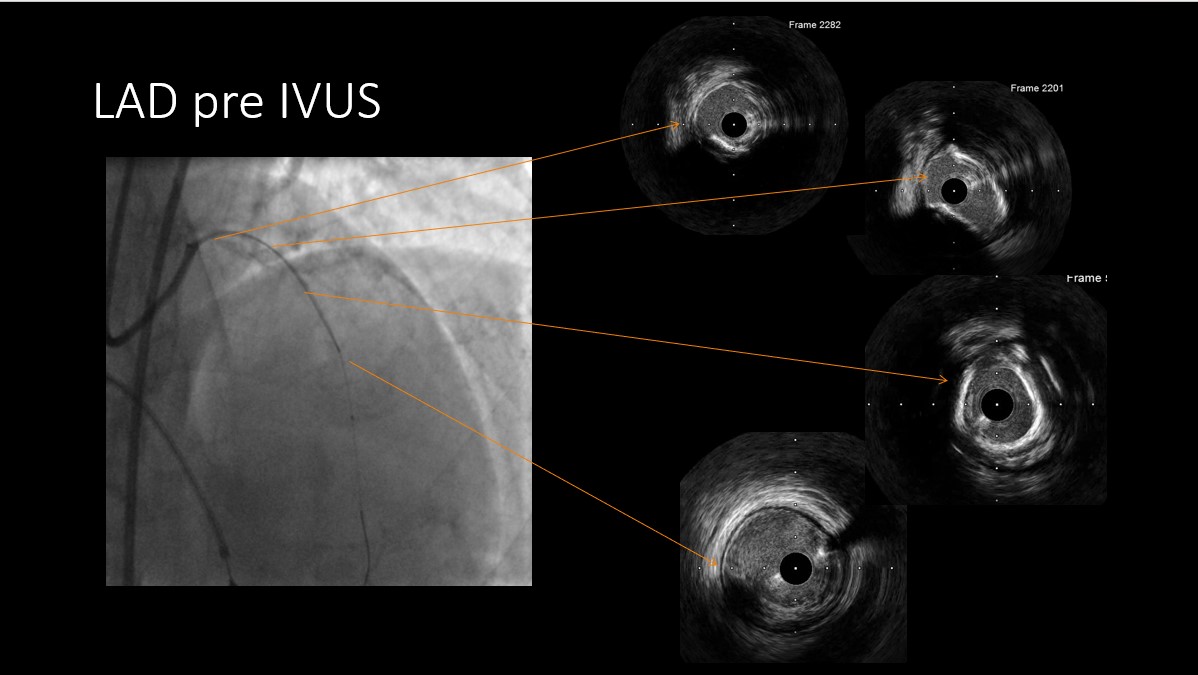
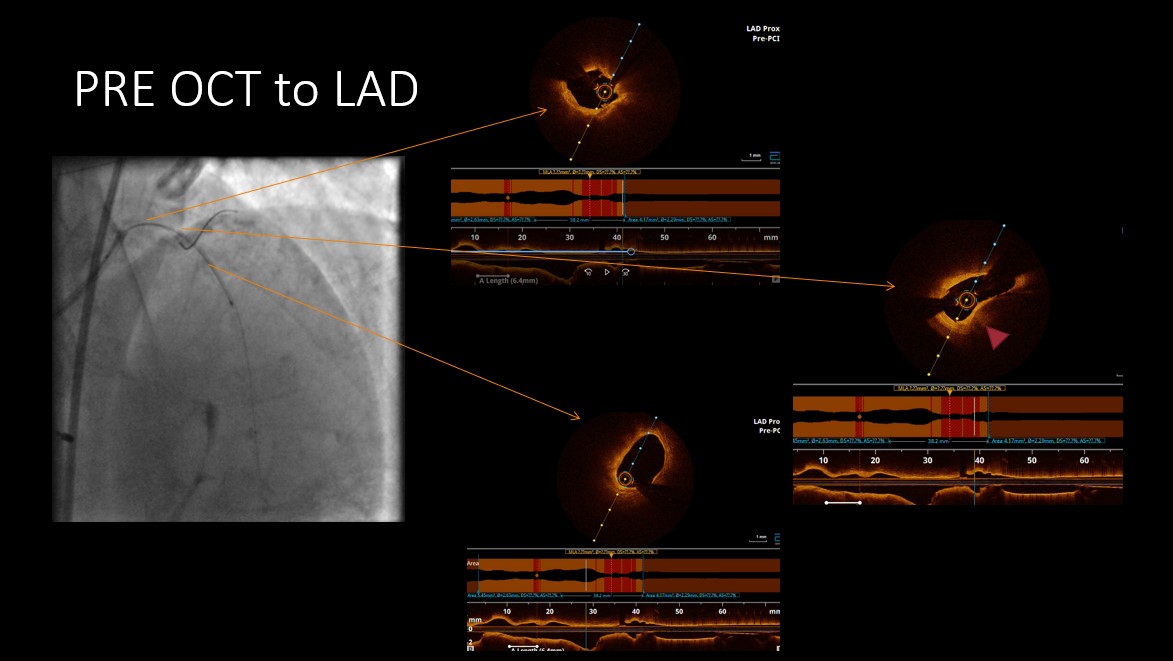
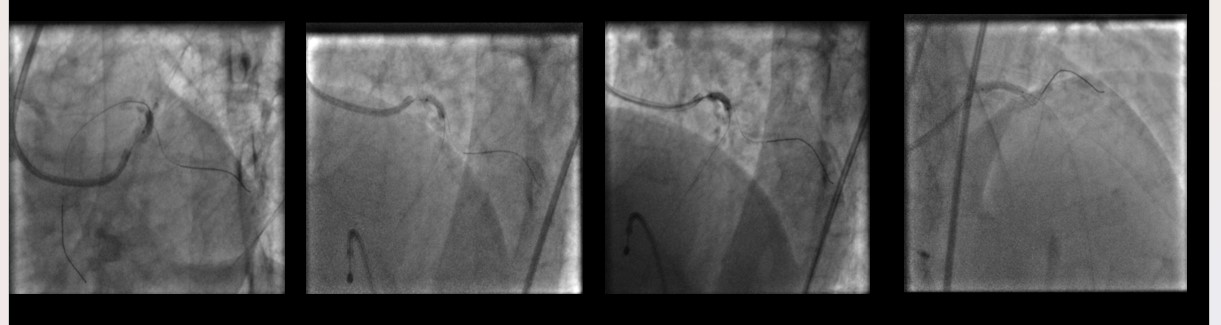
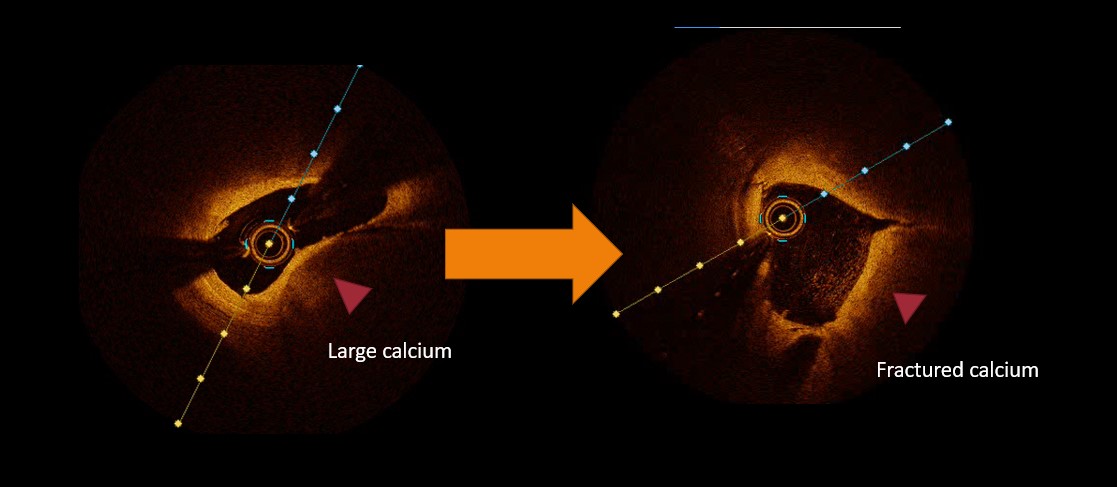
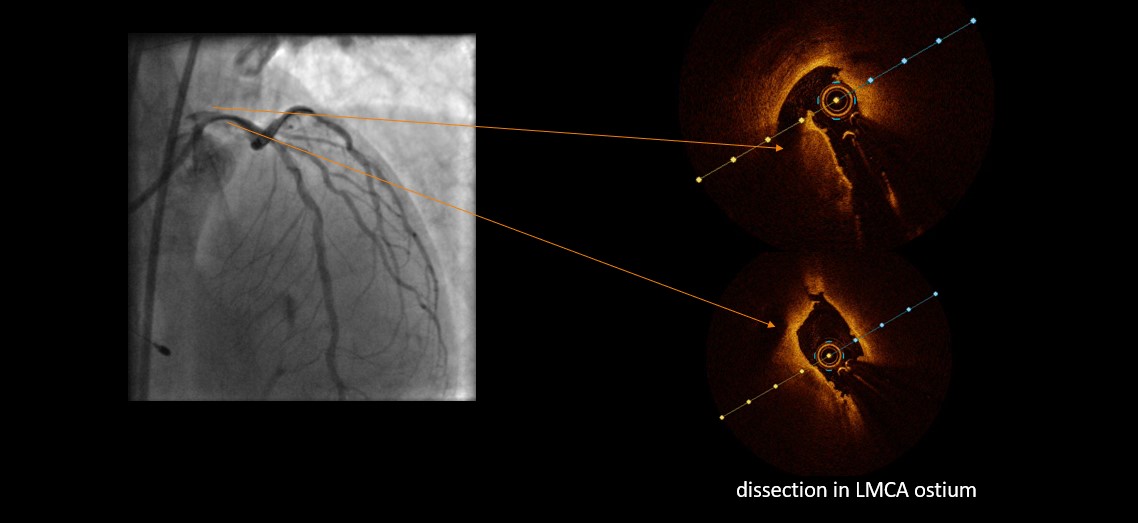
Tortuous RCA was engaged with 7F JR 3.5. Pre-dilatation ballons could be deployed only using guide extension catheter( 2.5 x15 and a 3.0x15 NC balloon at 16,18,20 atm ). over guidezilla support, two overlapping stents were deployed in the mid-RCA and proximal RCA measuring 2.75x30mm and 3x23mm DES respectively. Post-stenting distal to the distal stent residual stenosis was noticed which was interrogated by IVUS and found to be significant.A third overlapping stent was placed in the mid-distal RCA measuring 2.75x18 mm DES. Final IVUS showed well-expanded stents. Next LMCA was engaged with a 7F JL 3.5.OCT done to the LAD showed a long segment calcific lesion involving the mid distal LAD showing large medial calcium and fibrocalcific plaque .predilatation to the LAD and LMCA done with 3.5x12 IVL ballon 10 cycles of 10 pulse given with intermittent balloon deflations between pulses,without significant hemodynamic compromise apart from one episode of transient bradycardia.post IVL OCT showed cracks in the calcium and dissection in the left main ostium .stenting done to the LAD with 3.5x38 DES.Post dilatation done into the LAD with 4x15 mm NC balloon up to the LMCA ostium .post stenting OCT showed well-expanded stent with good apposition and adeqaute MSA.

Case Summary
Ostial left main and shaft disease with medial calcification presents a unique case for the application of intravascular lithotripsy to achieve good bed preparation and adequate stent expansion. Apprehensions regarding prolonged occlusion of LMCA during sustained bursts of lithotripsy can be overcome by using shorter bursts followed by deflating balloons intermittently to allow perfusion to the left system and ensuring RCA support is adequate prior to managing the LAD. The use of OCT was found to be useful to gauge the depth of calcium and determine the IVL balloon size.