
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-186
A Challenging Case Report: Transapical Vascular Plug to Occlude Large Pseudoaneurysm of the Mitro-Aortic Intervalvular Fibrosa (P-MAIVF) In Recurrent Prosthetic Valve Endocarditis
By Panupong Pota, Tasalak Thonghong, Noppon Taksaudom
Presenter
Panupong Pota
Authors
Panupong Pota1, Tasalak Thonghong1, Noppon Taksaudom1
Affiliation
Chiang Mai University, Thailand1,
View Study Report
TCTAP C-186
STRUCTURAL HEART DISEASE - Others (Structural Heart Disease)
A Challenging Case Report: Transapical Vascular Plug to Occlude Large Pseudoaneurysm of the Mitro-Aortic Intervalvular Fibrosa (P-MAIVF) In Recurrent Prosthetic Valve Endocarditis
Panupong Pota1, Tasalak Thonghong1, Noppon Taksaudom1
Chiang Mai University, Thailand1,
Clinical Information
Patient initials or Identifier Number
3910698
Relevant Clinical History and Physical Exam
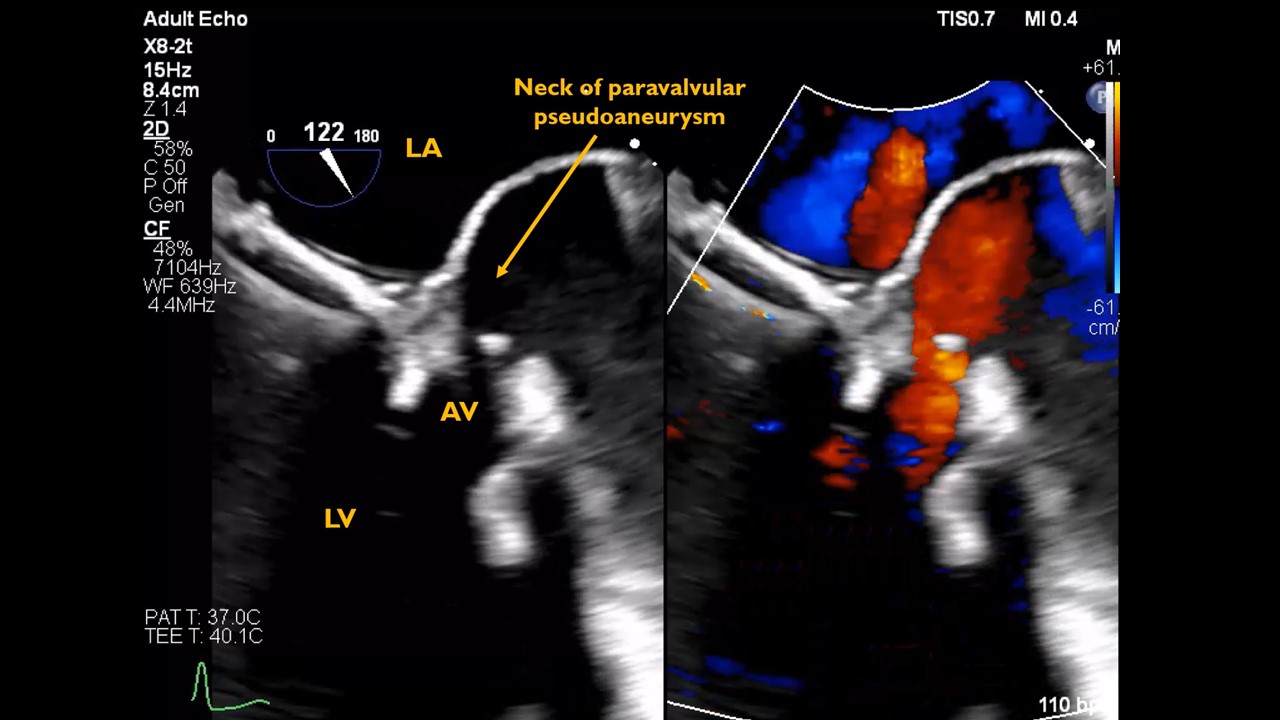
A 34-year-old man with congenital factor XI deficiency (Hemophilia C). He was diagnosed with severe AR from flail of RCC since 2018. He underwent AVR by On-X, MV repair. A follow-up TTE showed good prosthetic valve function, no leakage. In June 2022, the patient presented with Streptococcus agalactiae PVE. Physical examination revealed febrile, wide pulse pressure, soft S1, DRM grade III at LPSB and PSM grade III at apex. Severe AR with AV prosthetic dehiscence and severe MR were observed by TEE
Relevant Test Results Prior to Catheterization
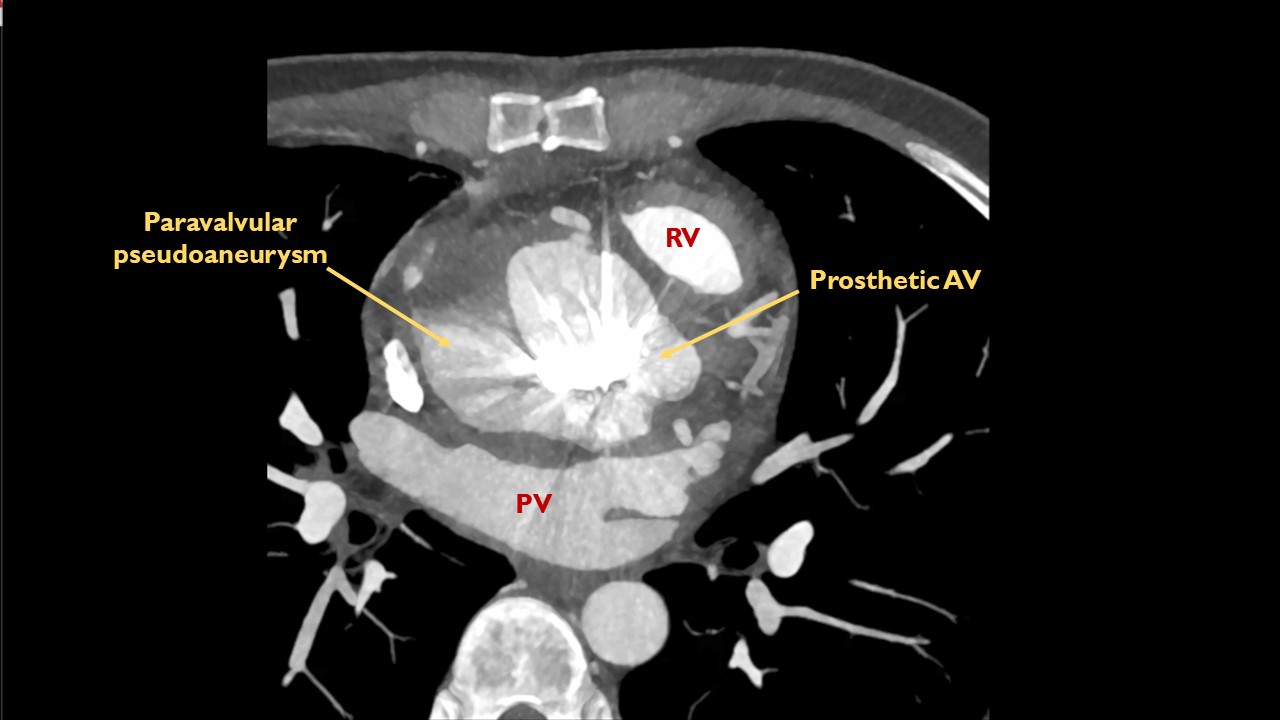
The heart team agreed to Redo AVR and MVR by ATS with reconstruction of MAIVF COMMANDO operation. Patient developed intraoperatively 5000 ml bleeding. a follow-up TEE showed active endocarditis with P-MAIVF. CT scan showed large P-MAIVF around metallic AVR, the largest one measured 5.9x3.5x6.5 cm. and size of aneurysmal neck was 1.8 cm. Heart team decided not to reoperate because of previous massive bleeding.Transcatheter vascular plug to occlude neck of pseudoaneurysmis considered alternatively
Relevant Catheterization Findings
Interventional Management
Procedural Step
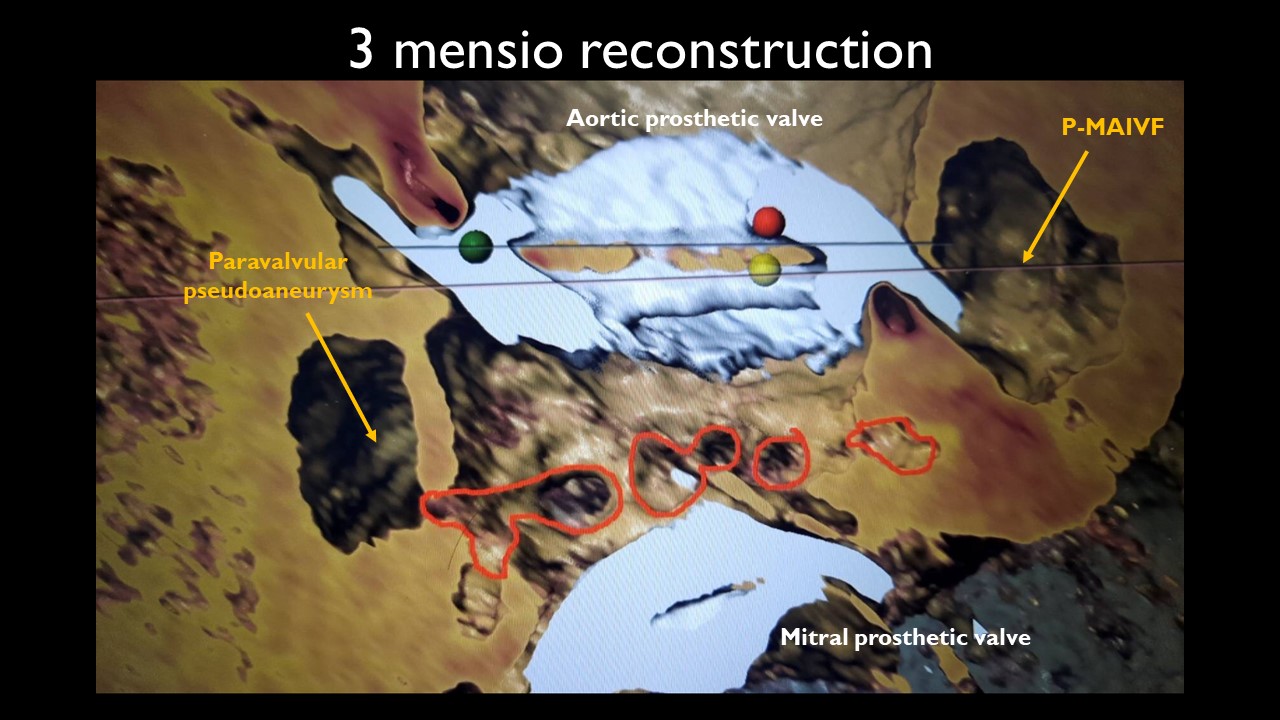
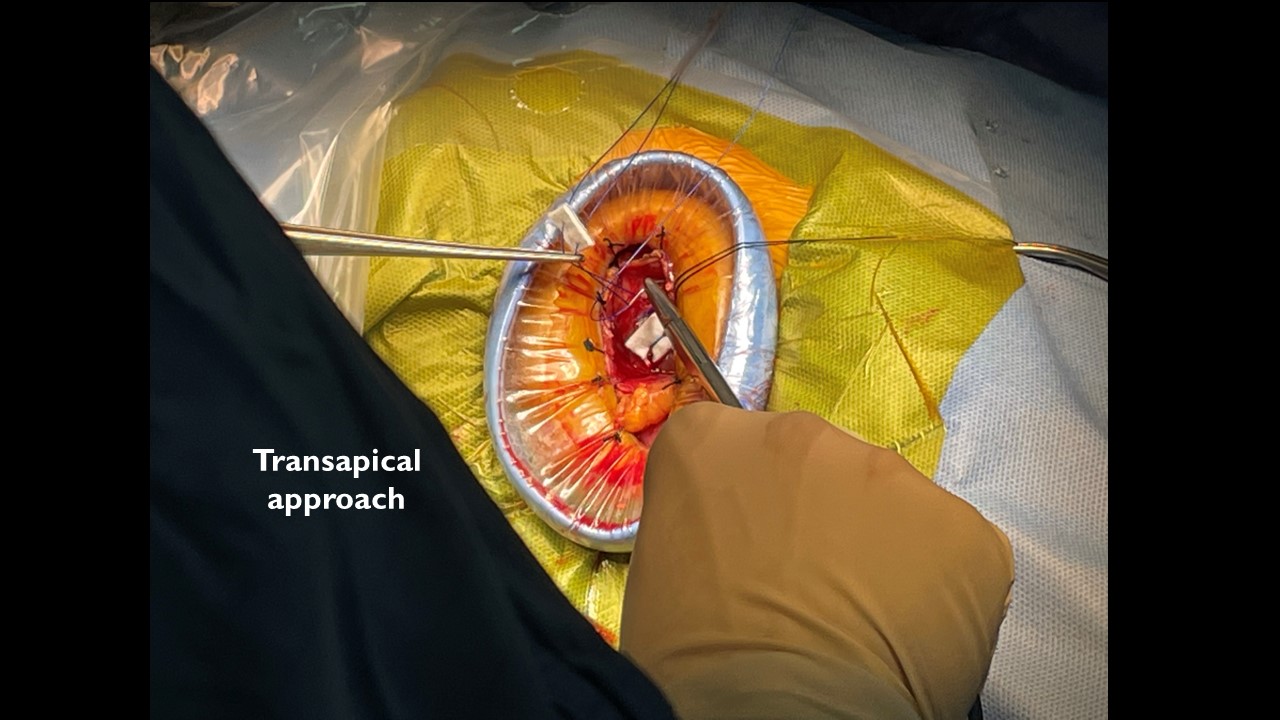
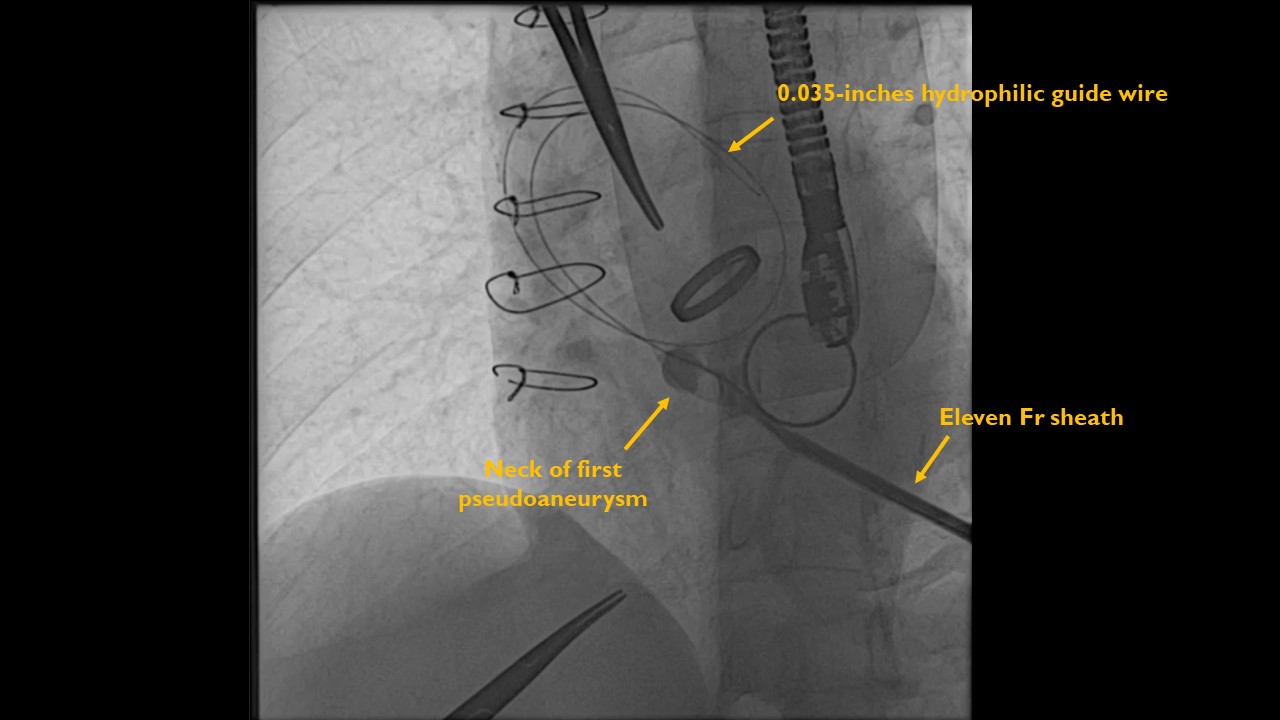
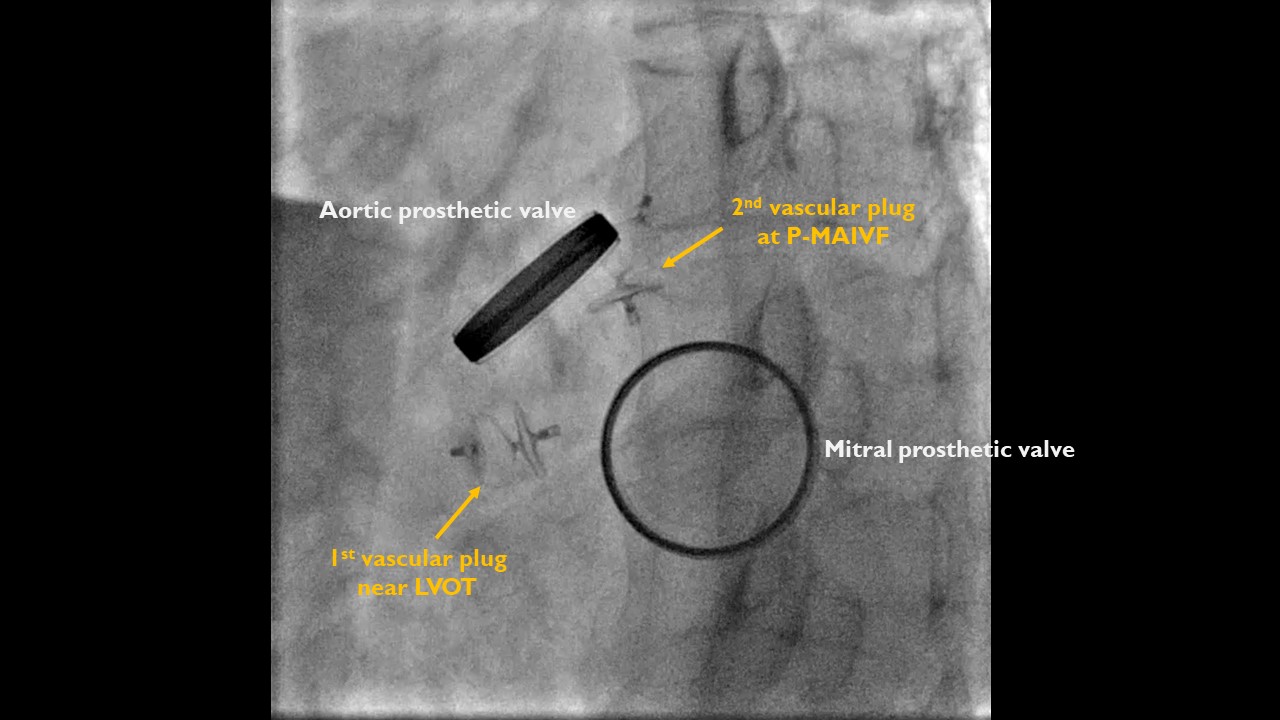
1. TEE revealed large two sites of flow across pseudoaneurysm. The first one was located adjacent to LVOT and the second one was close to MAIVF and the pulmonic valve.2. Left anterior mini-thoracotomy was performed as TAVI transapical approach.3.A purse string suture was appliedto reveal the apex.4. A pigtail catheter was inserted above AV prosthetic valve to perform a contrast injection to find the supra-valvular entry site and resulting in no supravalvular entry site.5. Eleven-Fr introducer sheath was inserted from the apex and contrast injection was performed to identify the sub-valvular entry site.6. 0.035-inches angled-tip hydrophilic guide wire was subsequently inserted into the neck of the pseudoaneurysm under TEE guided.7. The curve of the JR 3.5 guiding catheter was manually modified to reinforce the delivery of the vascular plug.8. First vascular plug No.10 was implanted near LVOT and TEE showed disappear of flow across the pseudoaneurysm connection.9. Using a similar procedure to find another sub-valvular entry site near MAIVF and pulmonic valve. The second vascular plug No.10 was subsequently implanted at MAIVF area. TEE showed decreasing flow across this pseudoaneurysm connection
Case Summary
Prosthetic valve endocarditis with complicated P-MAIVF is a critically concerned. The previous reports demonstrated a high mortality rate especially P-MAIVF > 3 cm. Surgical correction remains the recommended treatment. Nevertheless, inoperable patients may be advantaged from close follow-up. There has not been reported that using device closure to close the neck of P-MAIVF. We demonstrated transcatheter vascular plug to occlude the neck of paravalvular pseudoaneurysm by apical approach that may be an alternative treatment in non-operable patient. However,short- and long-term imaging and echocardiography follow-ups are necessary.Future prospective studies are also particularly needed.