
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-045
Successful Primary Angioplasty of Highly Calcific RCA With Multiple Lesions Followed by Staged PTCA of Highly Calcified Proximal LAD Using Cutting Balloons.
By Saurabh Goel
Presenter
Saurabh Goel
Authors
Saurabh Goel1
Affiliation
Wockhardt Hopsital, Mumbai Central, India1,
View Study Report
TCTAP C-045
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Successful Primary Angioplasty of Highly Calcific RCA With Multiple Lesions Followed by Staged PTCA of Highly Calcified Proximal LAD Using Cutting Balloons.
Saurabh Goel1
Wockhardt Hopsital, Mumbai Central, India1,
Clinical Information
Patient initials or Identifier Number
R K
Relevant Clinical History and Physical Exam
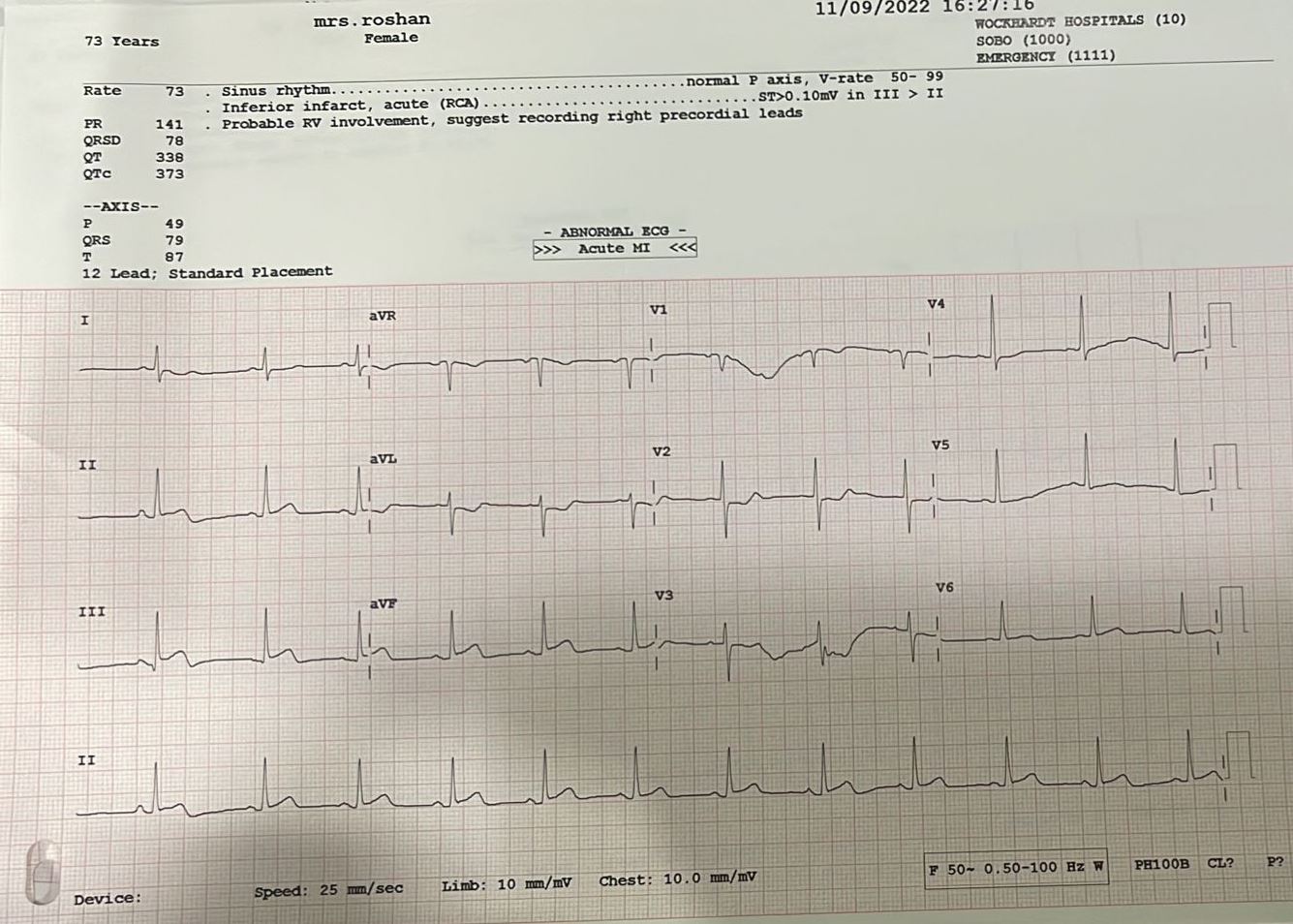
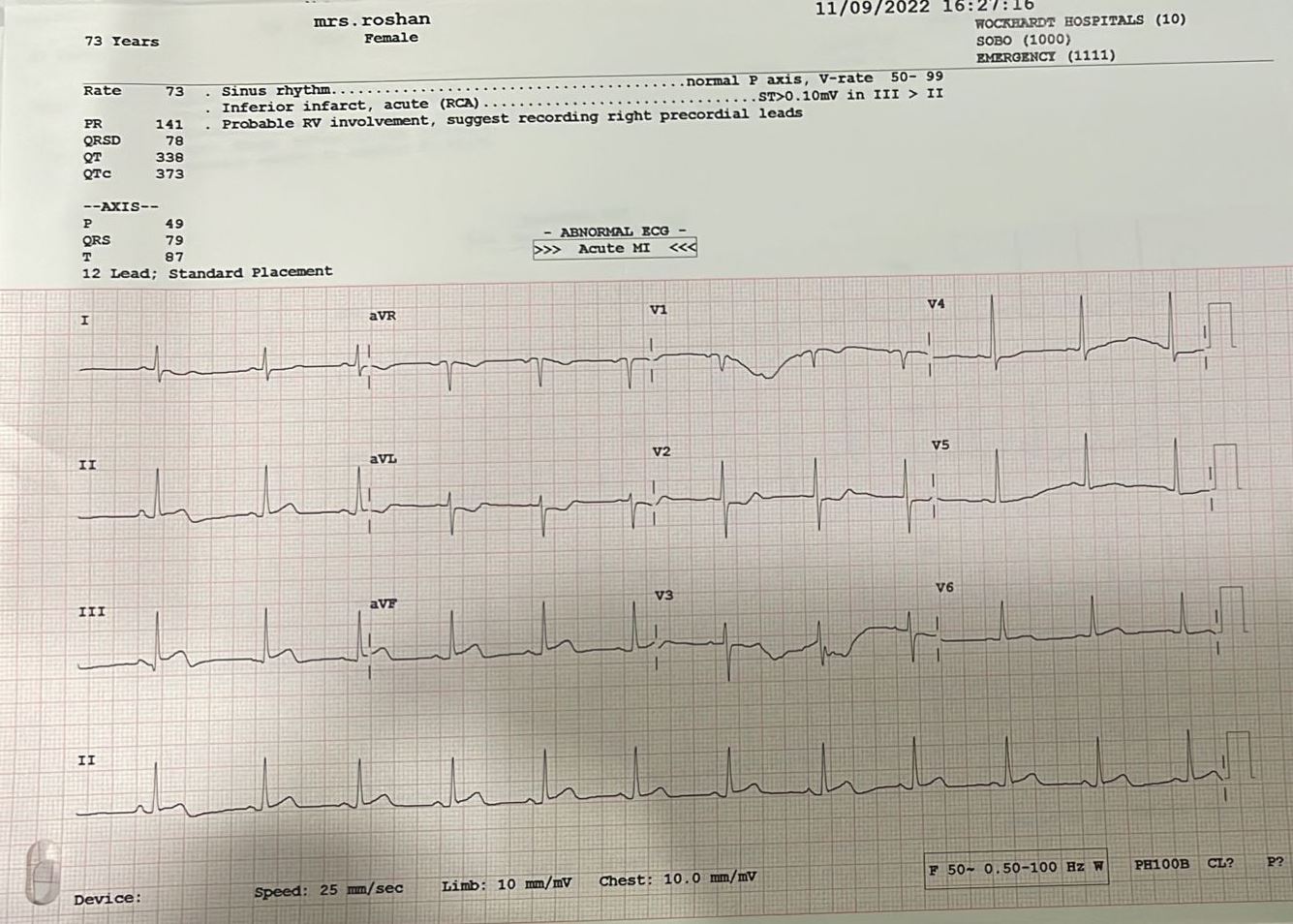
A 73 year old female , MRS R K, presented to Emergency Room with history of acute complaints of breathlessness and chest pain of two hours duration . ECG showing acute ST elevation Inferior Myocardial infarction. She had past history of NIDDM since 6 years with no history of hypertension or ischemic heart disease in past.
Relevant Test Results Prior to Catheterization
ECG –showed Inferior myocardial infarctionwith ST elevation in 2,3, AVF
Relevant Catheterization Findings
Angiographywas done from right femoral route and right venous sheath was also placed.



Interventional Management
Procedural Step
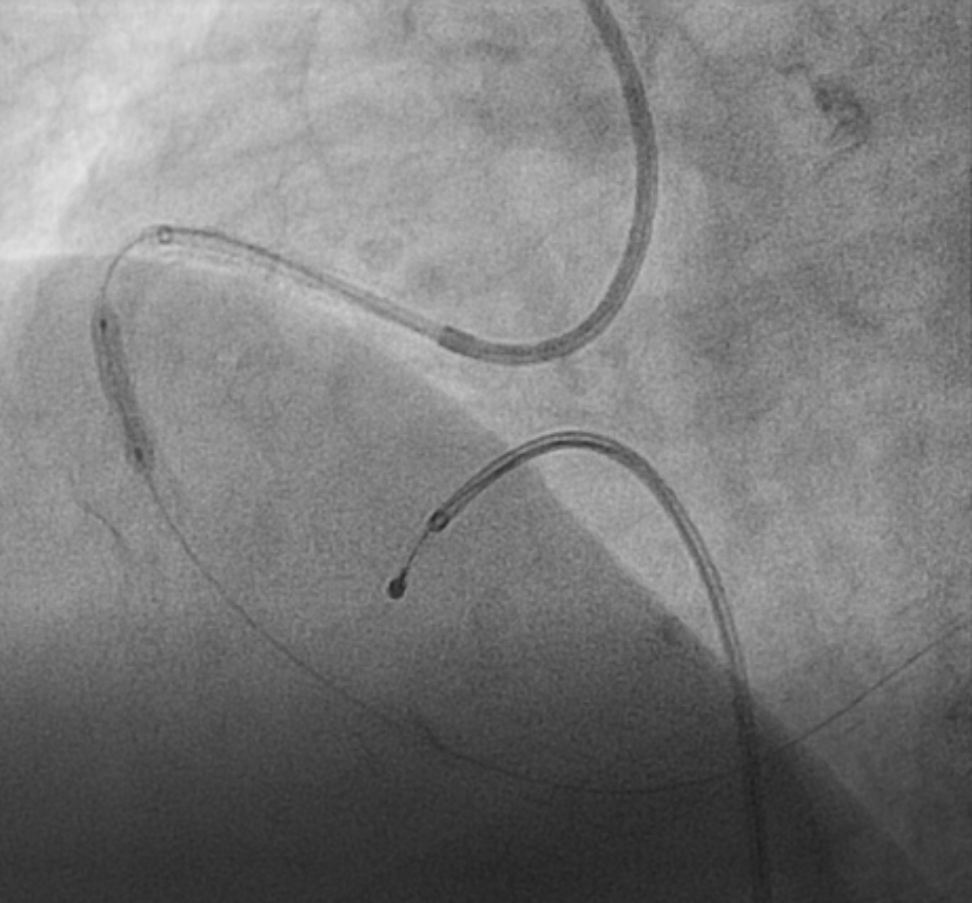
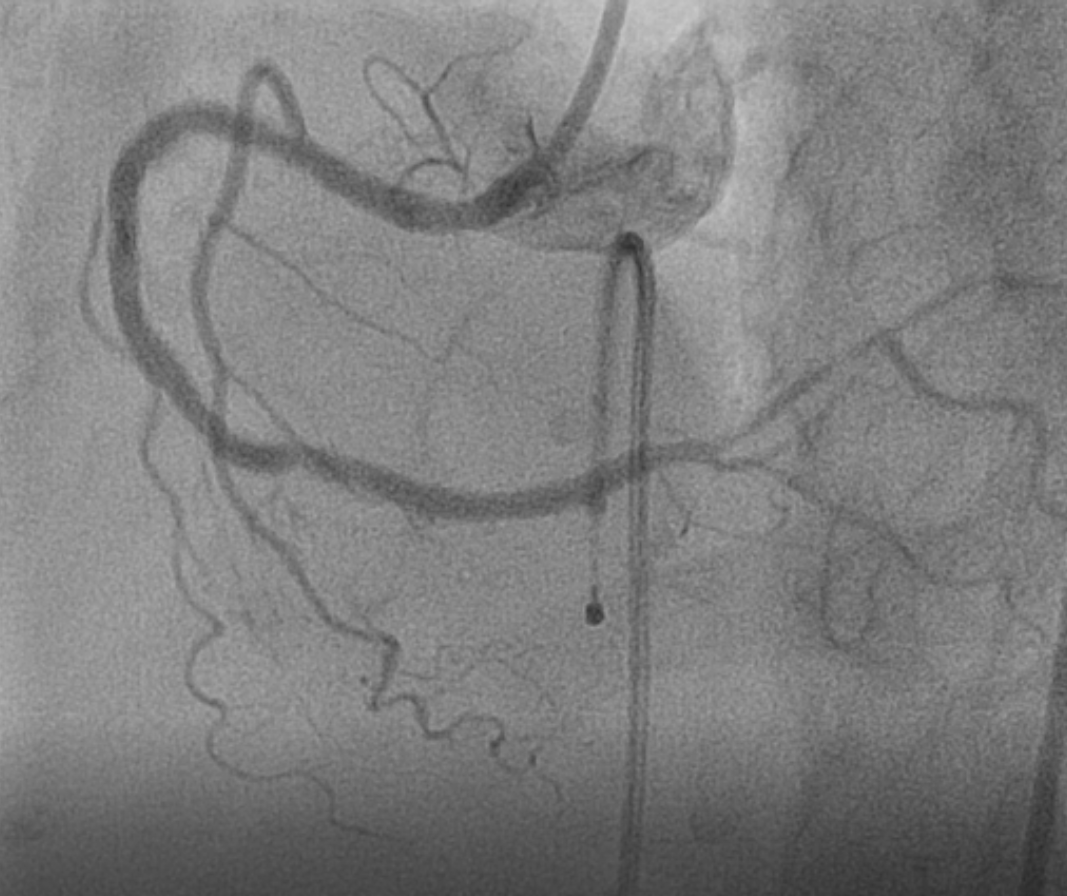
Urgent primary angioplasty of RCA was taken up and LAD was planned as staged PCI. The right coronary artery was cannulated using 6F JR 4 guiding catheter . the RCA lesions were crossed with Turn Trak wire , however due to heavy calcification, balloon could not be tracked beyond mid RCA . Hence predilatation of proximal lesion was done using 2.5 X 15mm N C trek balloon. This was followed by slows flow ,transient bradycardia and sustained ventricular tachycardia. Urgent D C cardioversion was done and pacing lead placed in RV . A 3.0 X 28 Xience Alpine Stent was urgently placed in osteoproximal RCA to keep the vessel open. Using guideliner support a balloon could then be advanced and the distal lesions were dilated. However the mid RCA lesion could not be dilated due to heavy calcification. Hence a Wolverine 2.75 X 12 balloon was used which could successfully dilate the lesion. Then using grand slam buddy wire for support, 2.75 X 33 Xience Alpine Stent was deployed in distal RCA overlapped by another 3.0 X 38 Xience Alpine Stent from mid to proximal RCA upto the proximal stent with good result.

Case Summary
This case demonstrates that in patients with acute myocardial infarction and highly complex calcified lesions, there is need for use of available technologies like cutting balloon and guide liner to achieve a satisfactory result. In an emergency situation of urgent primary angioplasty , the culprit infarct related vessel has to be revascularized ,however complex the lesions are. In this case of acute myocardial infarction with highly calcified complex RCA having multiple lesions, successful PTCA was done for RCA using guideliner, cutting balloon and multiple stents, and the patient made a complete uneventful recovery. Staged PTCA of calcified LAD was performed , also using a cutting balloon.