
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-051
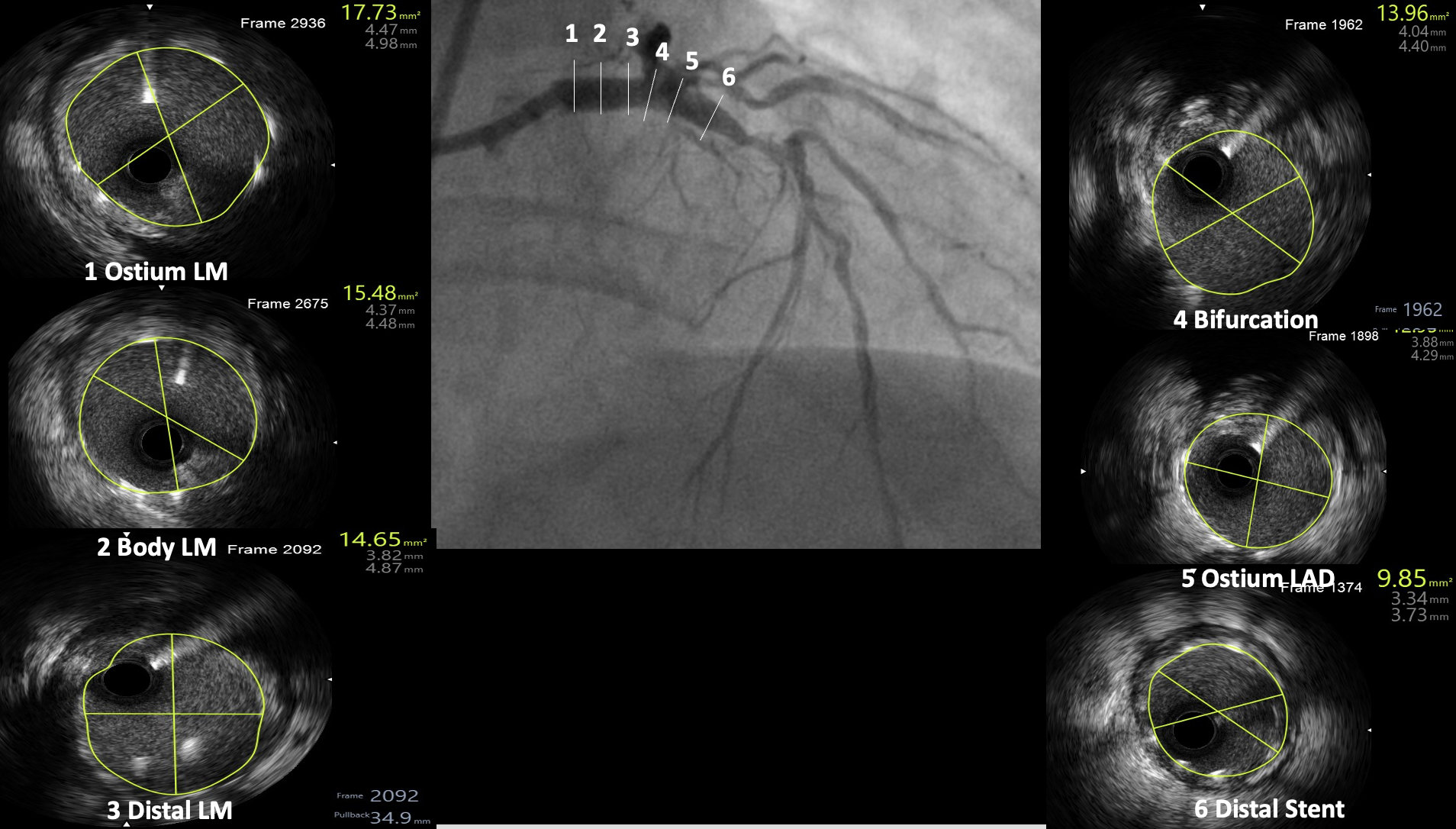
No Time for Surgeon an Emergency Critical Left Main Primary PCI Using IVUS
By Vijayendran Rajalingam, Dharmaraj Karthikesan, Saravanan Krishinan, Kantha Rao Narasamuloo, Kai Soon Liew, Yuen Hoong Phang, Chee Tat Liew, Tamim Ansari Bin Jahubar Sathik, Pirevina Naidu Krishnan Naidu, Nur Asmalina Binti Azizan, Izzatul Nadzirah Binti Ismail, Ahmad Faiz Mohd Ezanee
Presenter
Authors
Affiliation
No Time for Surgeon an Emergency Critical Left Main Primary PCI Using IVUS
Vijayendran Rajalingam1, Dharmaraj Karthikesan2, Saravanan Krishinan3, Kantha Rao Narasamuloo4, Kai Soon Liew4, Yuen Hoong Phang4, Chee Tat Liew5, Tamim Ansari Bin Jahubar Sathik2, Pirevina Naidu Krishnan Naidu2, Nur Asmalina Binti Azizan2, Izzatul Nadzirah Binti Ismail2, Ahmad Faiz Mohd Ezanee2
Sultan Idris Shah Serdang Hospital, Malaysia1, Hospital Sultanah Bahiyah, Malaysia2, Ministry of Health Malaysia, Malaysia3, Sultanah Bahiyah Hospital, Malaysia4, Pantai Penang Hospital, Malaysia5,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Relevant Test Results Prior to Catheterization
Echocardiography showed EF 50% , preserved wall thickness
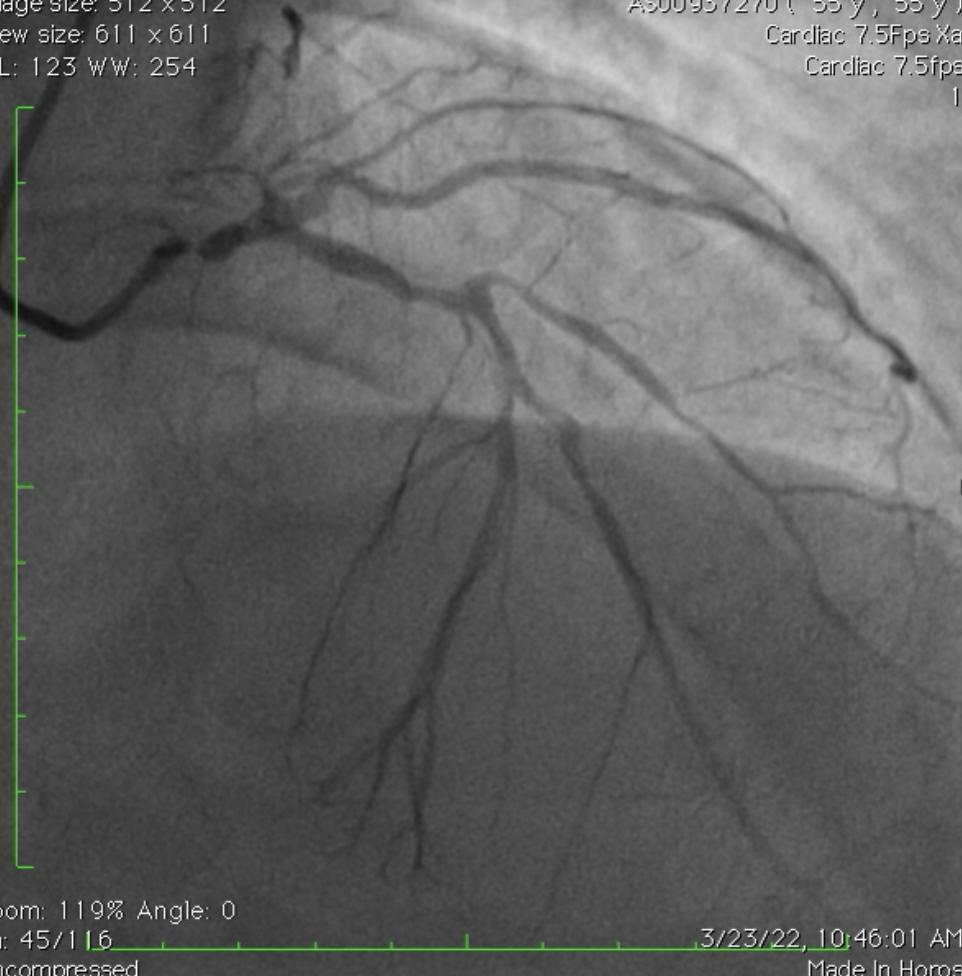
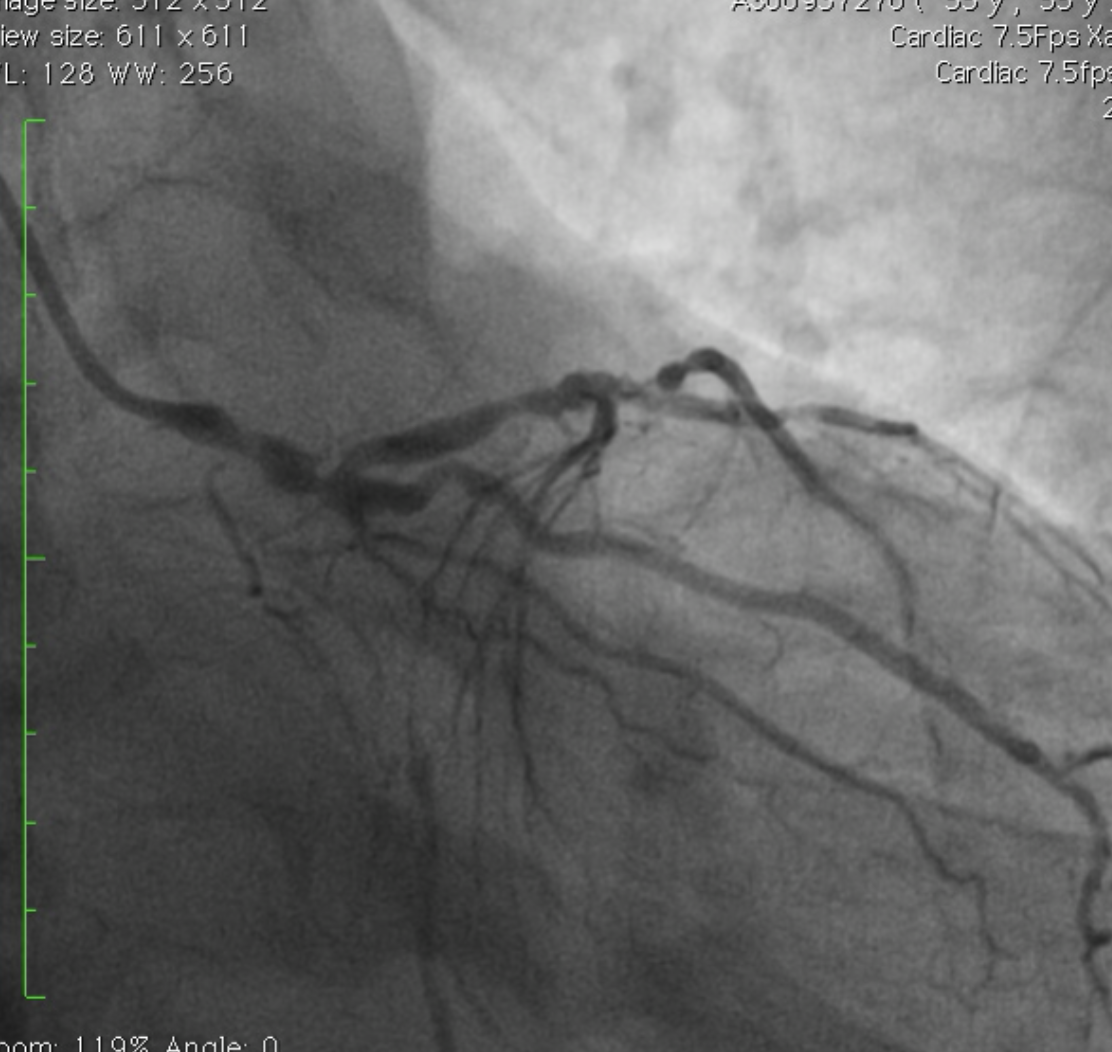
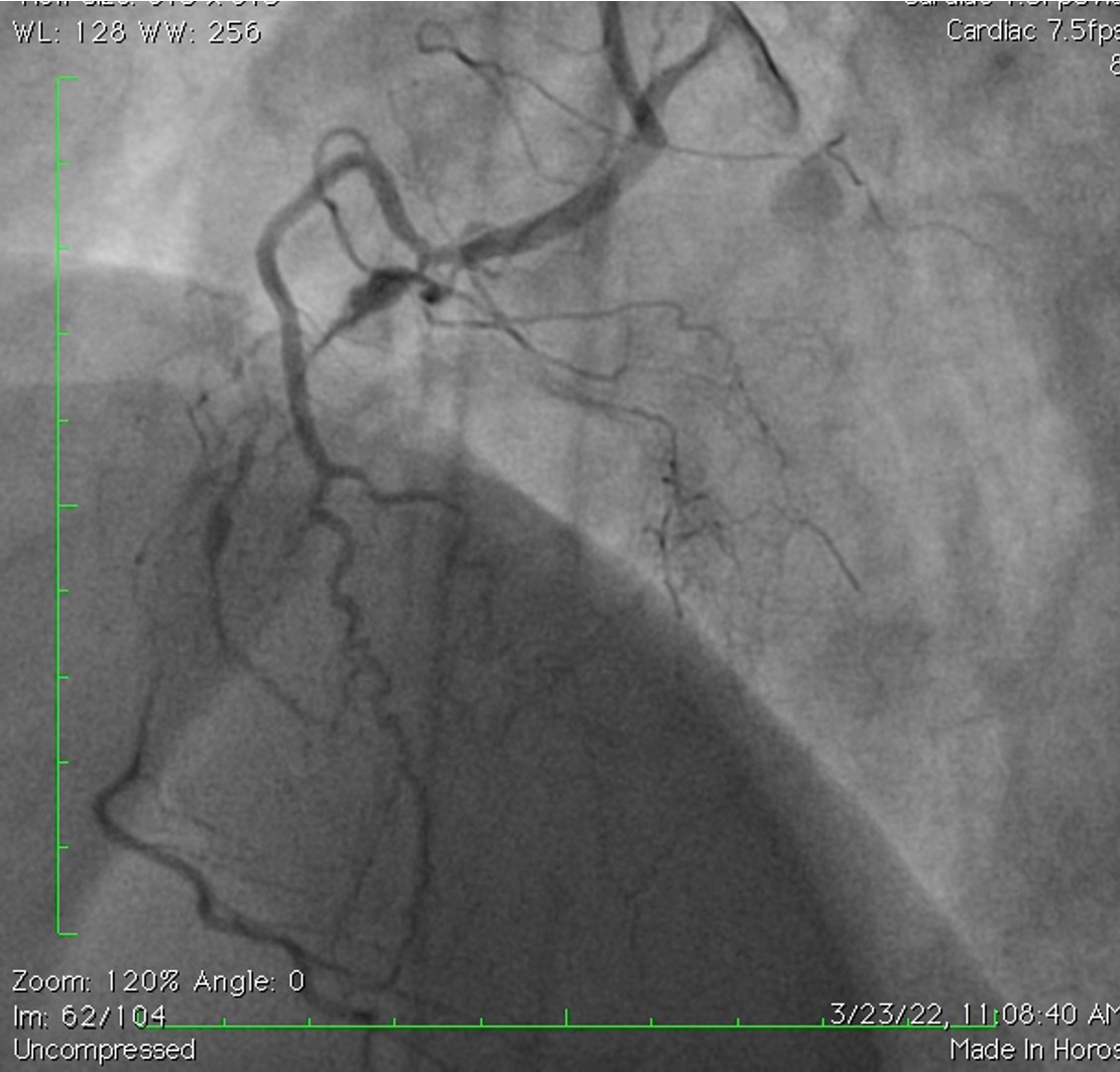
Relevant Catheterization Findings
Summary Severe 3VD with High Synthax score Plan for Urgent Inpatient bypass surgery (CABG )
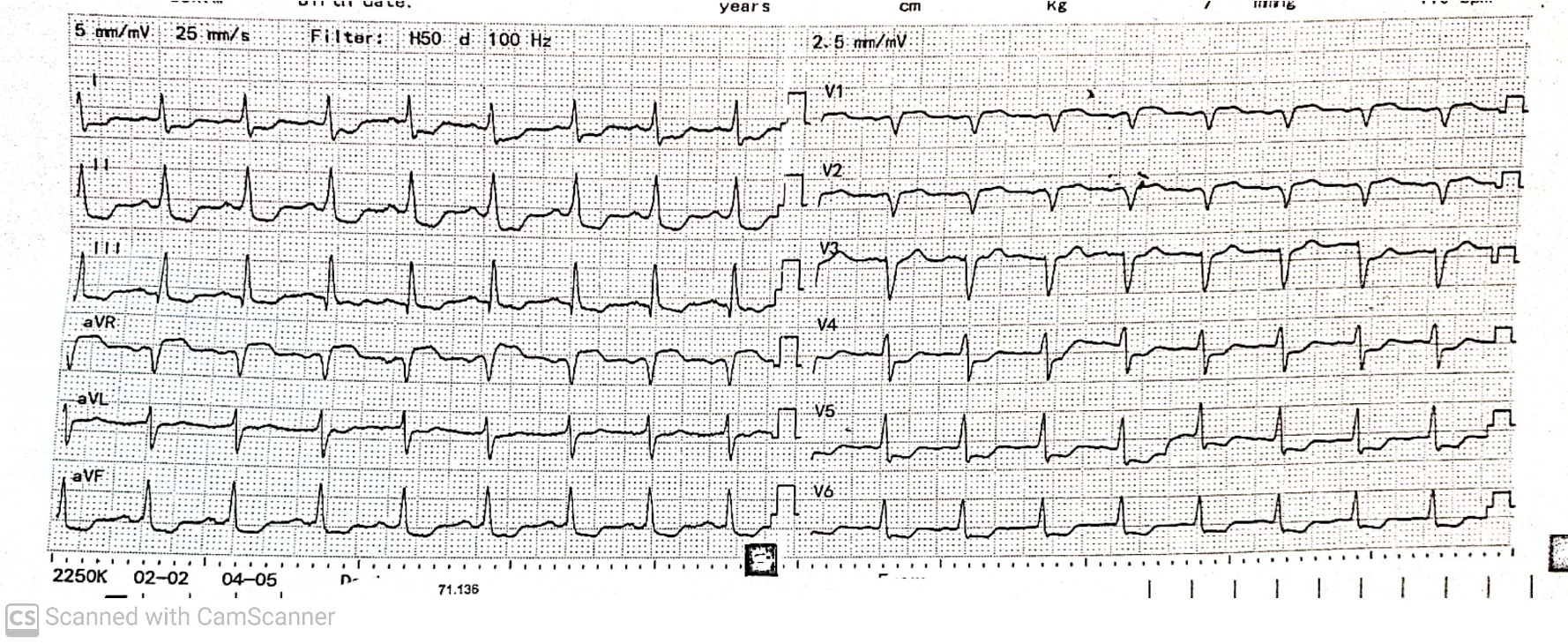
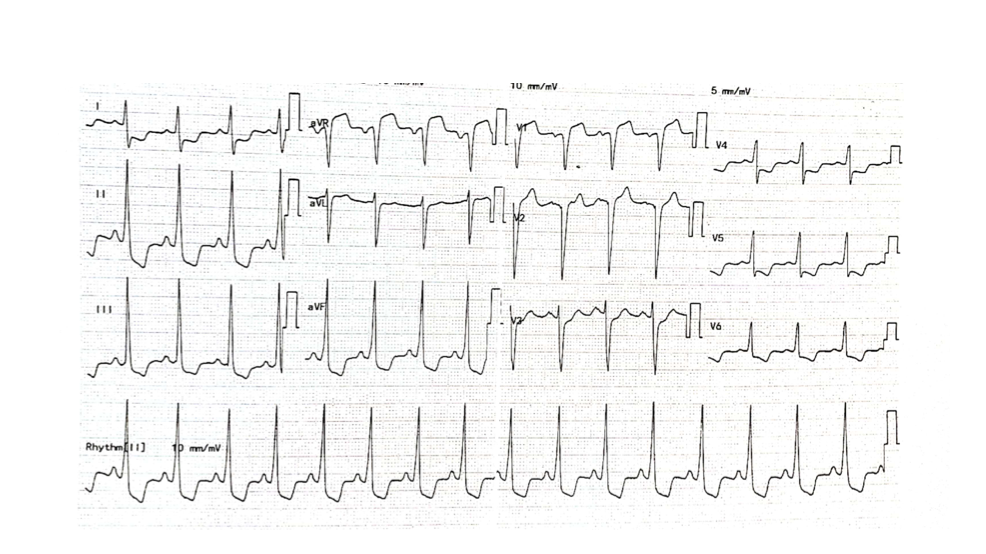
however at recovery bay while awaiting bed for admission patient developed sudden chest pain ,became less responsive with ECG changesdecided for urgent Primary Left main Revascularization as we do not have an inhouse cardiac surgeon
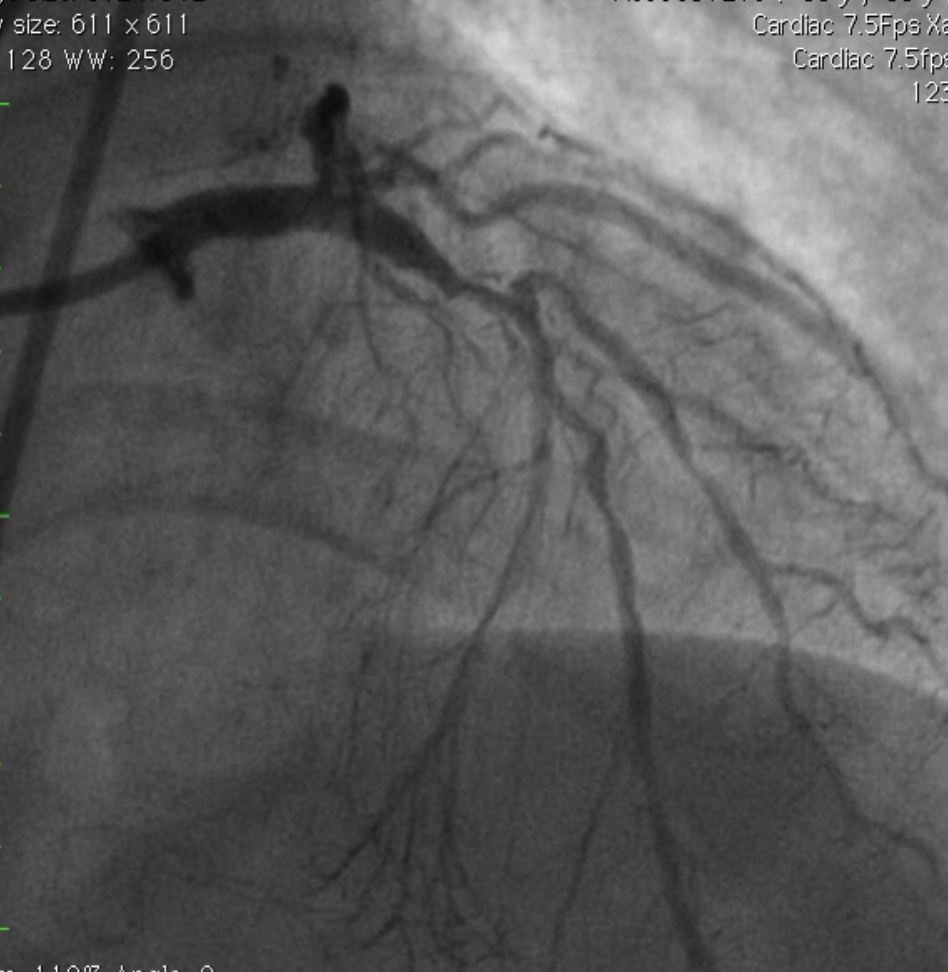
Interventional Management
Procedural Step
Post procedure he remained well Inotropes weaned off no chest pain ,ambulating discharged home 48hours later because we have arranged for an Urgent CTCA to assess the RCA anomaly

Case Summary
2. Operator Experience and Expertise with imaging is important to get equivalent to a CABG like outcome
CTCA confirm RCA is anomalous arising from Left coronary cusp with low interatrial course and mRCA CTO with ipsilateral collateral.He has quit smoking and remained asymptomatic till today and is on Guideline Directed Medical Therapy and is back to his routine job as a Rubber Tapper.