
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-003
The Slow, the Silent and the Deadly: Delayed Onset Acute Myocardial Infarction Due to Left Main Occlusion Following Motor Vehicle Accident Without Obvious Chest Trauma
By Siew Hoon Ong, Khai Chih Teh, Yee Sin Tey, Rhuban Sundran, Mohd Nasir Muda
Presenter
Siew Hoon Ong
Authors
Siew Hoon Ong1, Khai Chih Teh1, Yee Sin Tey1, Rhuban Sundran1, Mohd Nasir Muda1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-003
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
The Slow, the Silent and the Deadly: Delayed Onset Acute Myocardial Infarction Due to Left Main Occlusion Following Motor Vehicle Accident Without Obvious Chest Trauma
Siew Hoon Ong1, Khai Chih Teh1, Yee Sin Tey1, Rhuban Sundran1, Mohd Nasir Muda1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
414834
Relevant Clinical History and Physical Exam
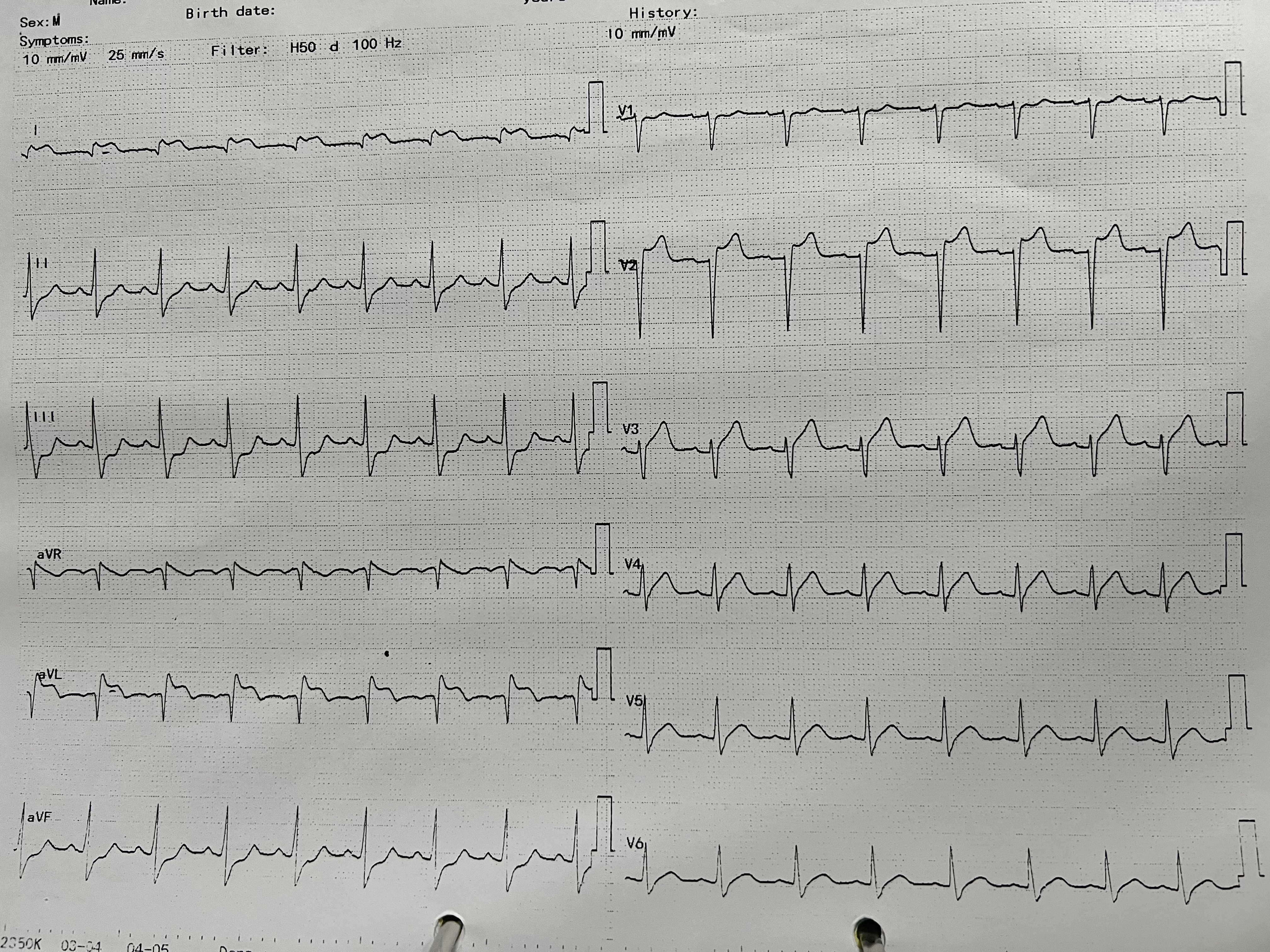
27 year old man, no known medical illness sustained motor vehicle accident (motorcycle vs lorry) with open fracture of left tibia plateau, loss of consciousness, retrograde amnesia and no recollection of mechanism of accident. Vitals were stable with no signs of chest trauma. 6 hours after the accident he developed chest pain with ECG showing ST elevation 1, aVL, V2 and V3 with reciprocal inferior ST depression. He was referred for primary PCI for acute anterolateral myocardial infarction.
Relevant Test Results Prior to Catheterization
blood pressure 110/62 mmHgheart rate sinus tachycardia 110 bpm
troponin T >10,000 pg/mlcreatinine 130 umol/lHb 15.6 g/dl
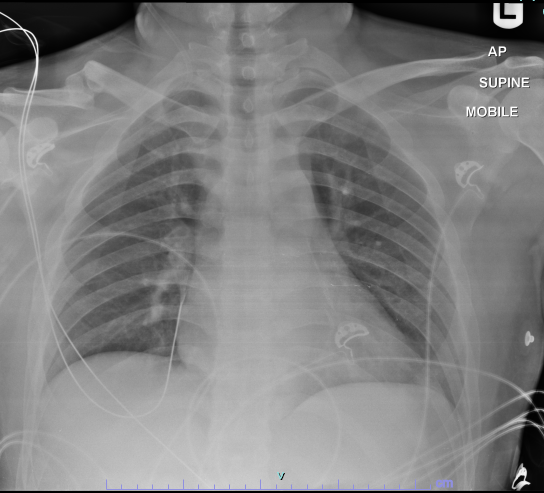
chest X ray: clear lung fields, no rib fracture or pneumo/ hydrothorax
ECG: ST elevation I, aVL, V2 and V3; reciprocal ST depression II, III, aVF
troponin T >10,000 pg/mlcreatinine 130 umol/lHb 15.6 g/dl
chest X ray: clear lung fields, no rib fracture or pneumo/ hydrothorax
ECG: ST elevation I, aVL, V2 and V3; reciprocal ST depression II, III, aVF
Relevant Catheterization Findings
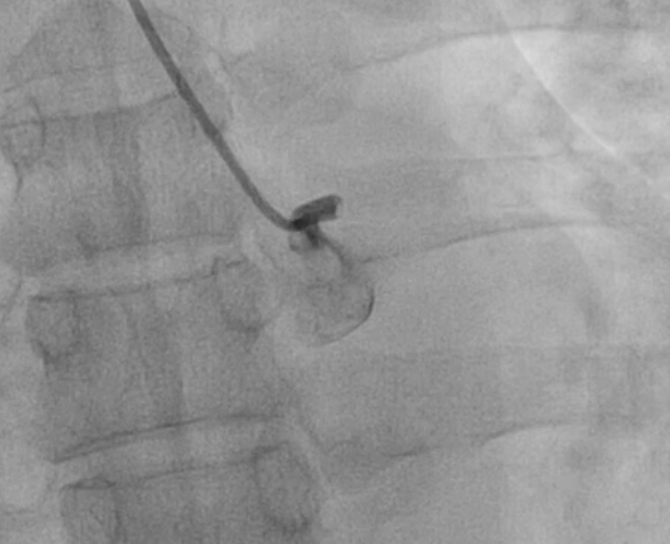
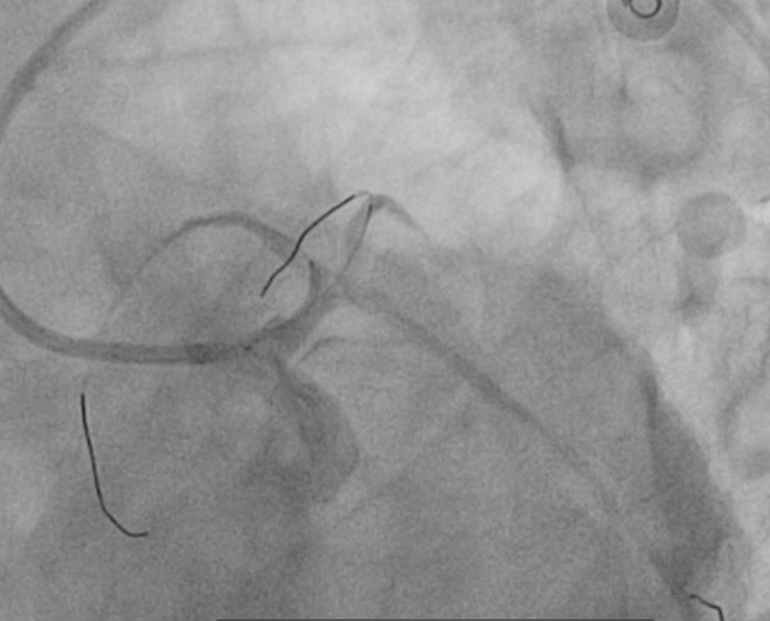
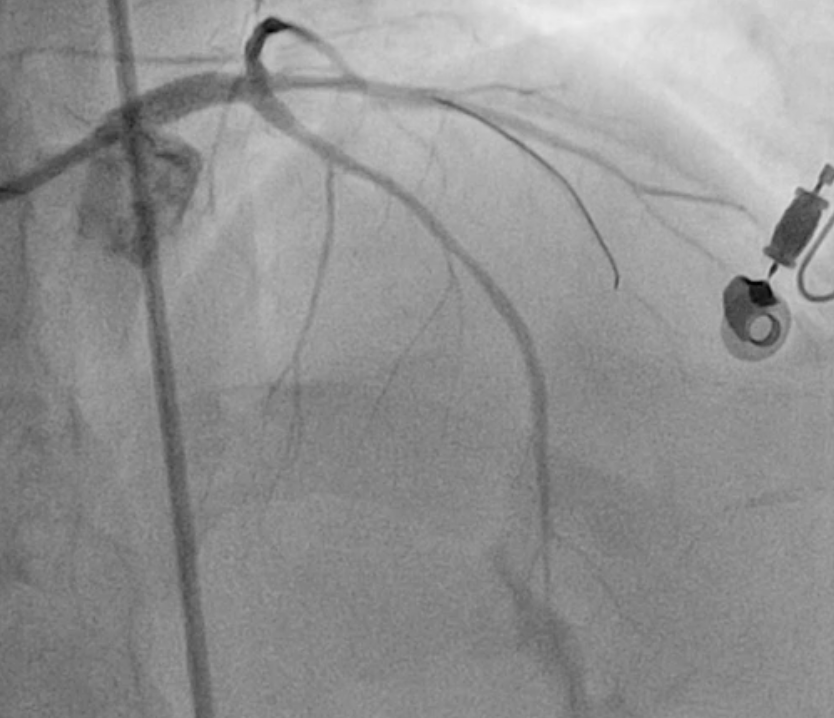
left main: acute total occlusion at proximal left main; left main body dissection with thrombus at distal LM after flow restored
right coronary: normal, taken after completion of left coronary angioplasty


right coronary: normal, taken after completion of left coronary angioplasty
Interventional Management
Procedural Step
Left main(LM) engaged with 6Fr EBU 3.5 guide, crossed occlusion with workhorse floppy wire
Left main occlusion was predilated with semi compliant (SC) 2.0 x 12mm balloon at high pressure 12-16mmHg atm.
Thrombus aspiration was performed twice, yielding copious red thrombus. Post aspiration cine revealed dissection flap at left main body with large thrombus occupying distal left main into proximal LAD, with underfilling of LAD to distal vessel. Left circumflex artery appeared normal.
Further predilatation with SC 2.5 x 15mm balloon was performed with wire protecting left circumflex artery and intermediate branch.
IVUS shows LM 4.5mm2 and LAD 3.5mm2 MLA with dissection flap at LM body.
We decided for ostium LM to proximal LAD stenting with RESOLUTE ONYX 3.5 x 18mm. Proximal optimisation of left main ostium was performed with 4.5 x 8mm NC balloon at 16 atm. Distal LM to proximal LAD was postdilated with a 4.0 x 8mm balloon at 10 atm.
Final results show TIMI III flow in all vessels.
Patient remained hemodynamically stable throughout procedure without requiring left ventricular output support. However following procedure he developed worsening dyspnoea and acute pulmonary edema requiring mechanical ventilation.

Case Summary
The patient developed acute pulmonary edema, nosocomial pneumonia, acute kidney injury and heart failure with reduced LVEF (EF 27%, global hypokinesia) requiring ventilation, inotropic support and prolonged intensive care. He made slow but stable recovery and was discharged.
This case illustrates left main occlusion, likely due to intimal tear and thrombus formation, causing delayed onset acute myocardial infarction 6 hours following possible blunt trauma during motor vehicle accident despite no signs of chest injury. High degree of suspicion of acute coronary syndrome following trauma, rapid transfer and prompt percutaneous intervention were the key steps to this patient's survival.
This case illustrates left main occlusion, likely due to intimal tear and thrombus formation, causing delayed onset acute myocardial infarction 6 hours following possible blunt trauma during motor vehicle accident despite no signs of chest injury. High degree of suspicion of acute coronary syndrome following trauma, rapid transfer and prompt percutaneous intervention were the key steps to this patient's survival.