
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-176
Percutaneous Coronary Intervention to Left Main and Left Anterior Descending Artery With Rotational Atherectomy via Left Distal Radial Access
By Meei Wah Chan, Benjamin Tao Xiung Lim, Abdul Raqib Abd Ghani, Kamaraj Selvaraj
Presenter
Meei Wah Chan
Authors
Meei Wah Chan1, Benjamin Tao Xiung Lim1, Abdul Raqib Abd Ghani1, Kamaraj Selvaraj2
Affiliation
Hospital Serdang, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2,
View Study Report
TCTAP C-176
OTHERS - Vascular Access (Transradial)
Percutaneous Coronary Intervention to Left Main and Left Anterior Descending Artery With Rotational Atherectomy via Left Distal Radial Access
Meei Wah Chan1, Benjamin Tao Xiung Lim1, Abdul Raqib Abd Ghani1, Kamaraj Selvaraj2
Hospital Serdang, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Madam HZ
Relevant Clinical History and Physical Exam
A 59 years old lady was referred from dialysis center for intradialytic chest pain and hypotension. She was treated for diabetes mellitus, hypertension and end staged renal disease on regular haemodialysis via right fistula. She presented with chest pain during dialysis for the past 2weeks associated with hypotension and difficulty in breathing. Her blood pressure was 180/90mmhg, heart rate 66bpm and saturation 99% . Lungs auscultation found basal crepitation , no murmur heard.
Relevant Test Results Prior to Catheterization
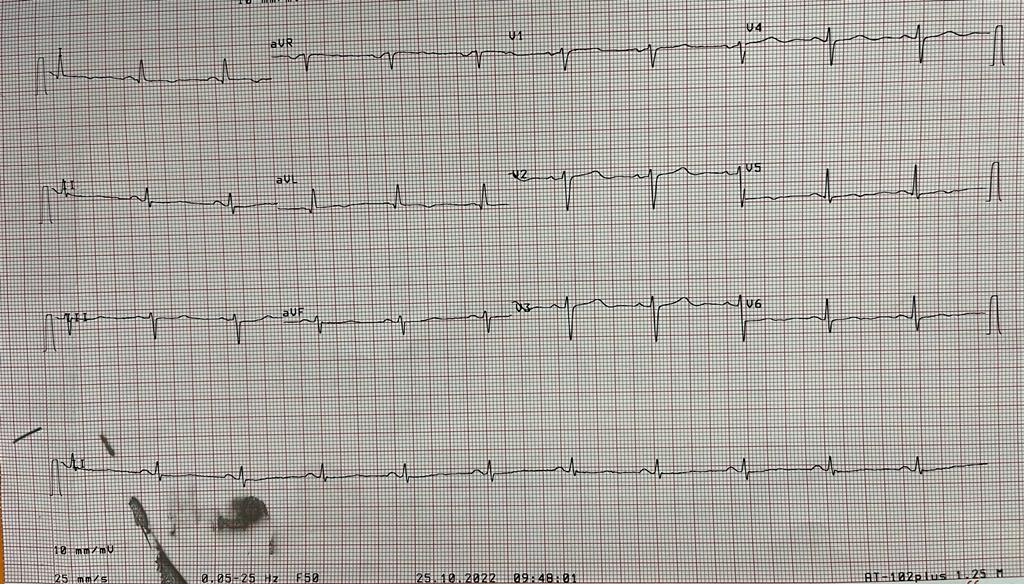
Her laboratory shown urea 14 mmol/l , creatinine 644 umol/, haemoglobin 19g/dl, Troponin I 127ng/l which was raised. Her electrocardiogram shown sinus rhythm , T wave inversion at lateral lead . She was treated for non-ST elevation myocardial infarction. Coronary angiography was performed on the next day of admission.
Relevant Catheterization Findings
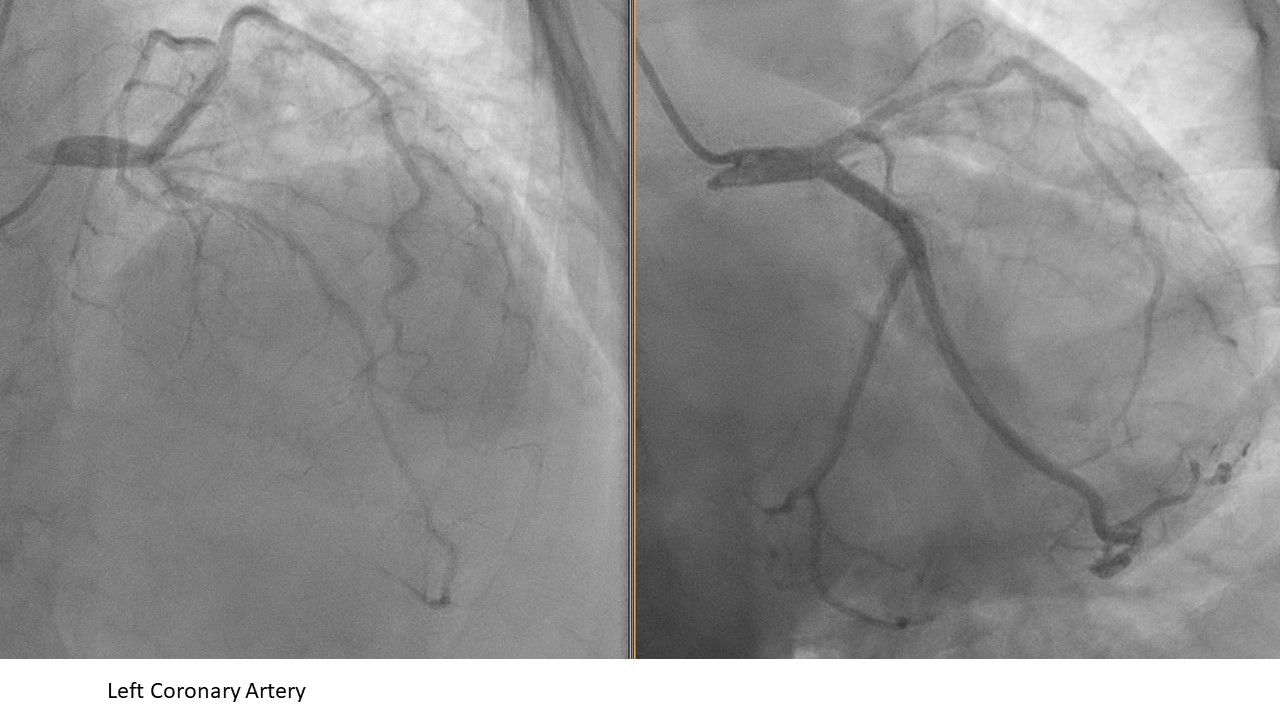
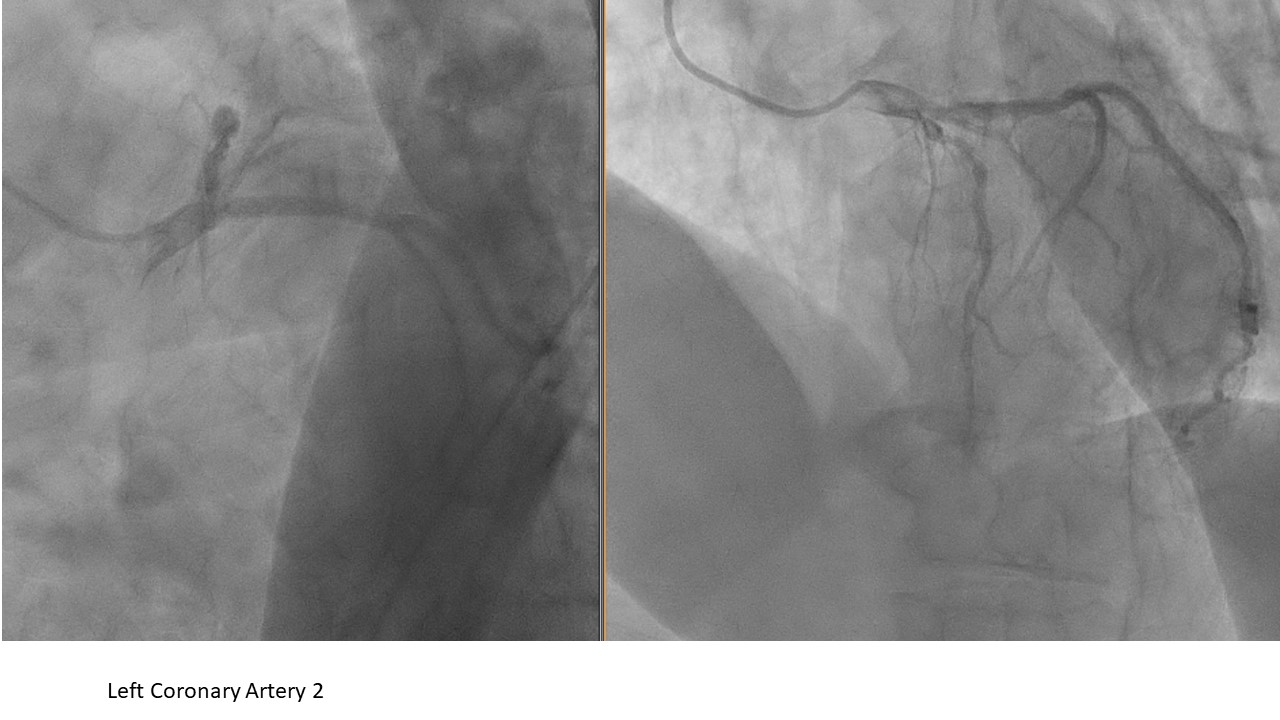
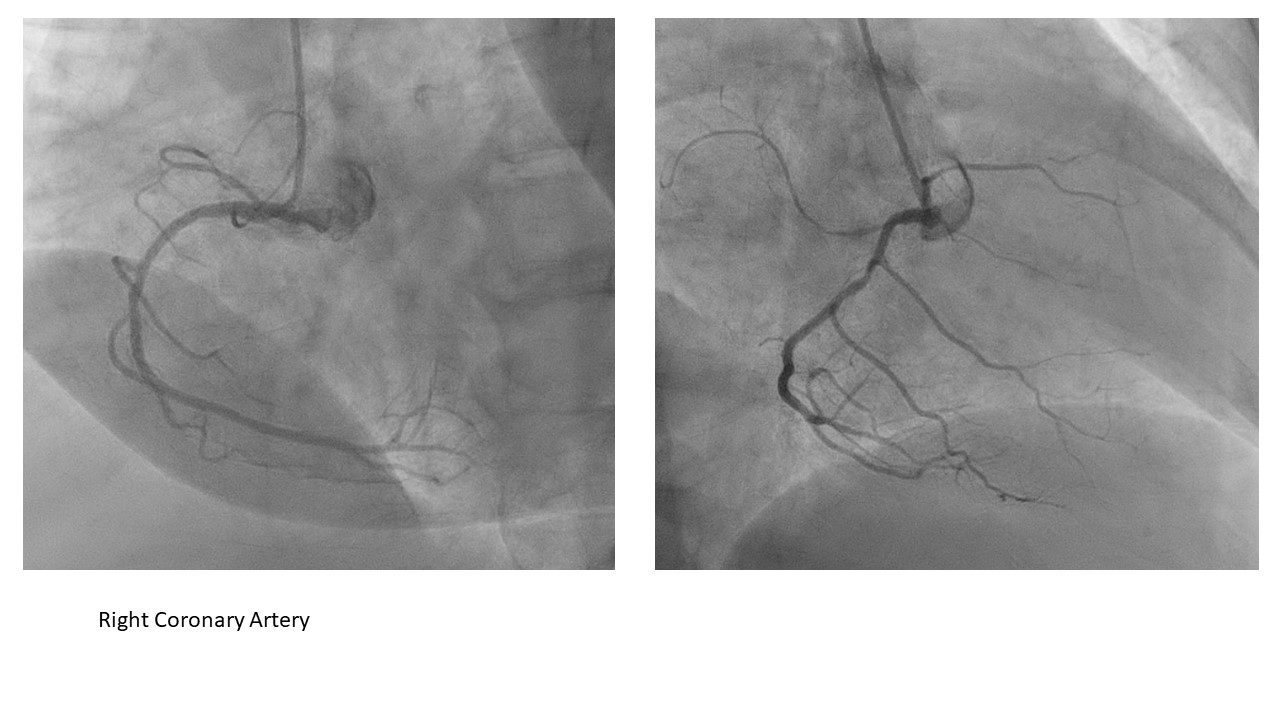
In view of the presence of fistula at right arm and high aPTT post haemodialysis with heparin , left distal radial artery was punctured at left snuffbox and 6Fr sheath was inserted. Coronary angiography done with JR 3.5 and JL 4.0 revealed co-dominant vessels, distal left main 20-30% stenosis, proximal LAD severe stenosis with heavily calcified vessel, distal LAD 50% stenosis. Normal LCx , and moderate lesion at RCA. Decision was made for angioplasty over the LM-LAD with rotational atherectomy.
Interventional Management
Procedural Step
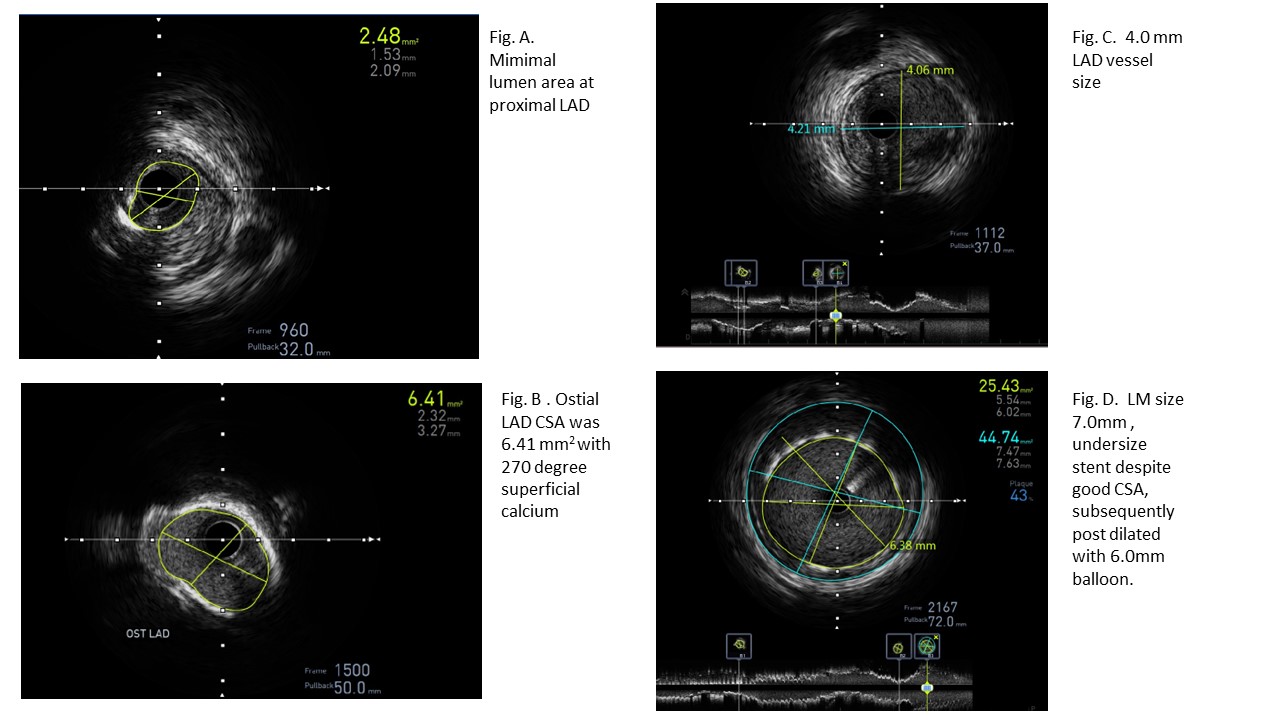
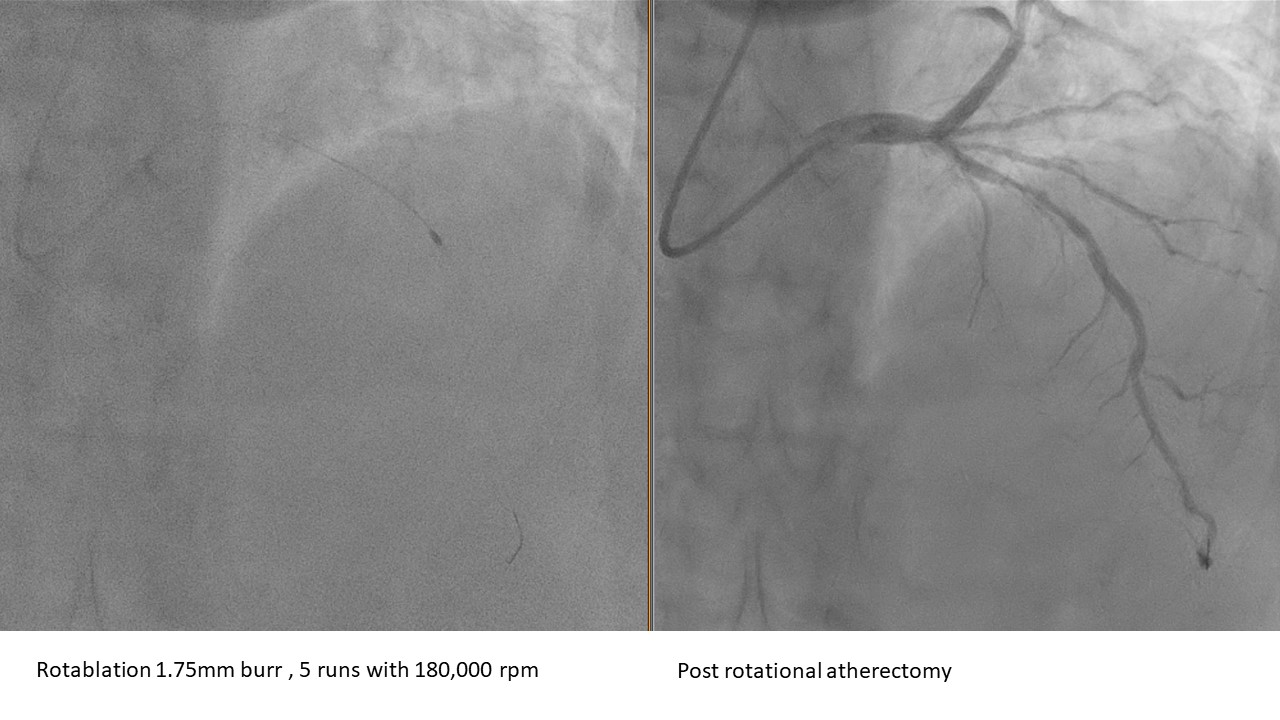
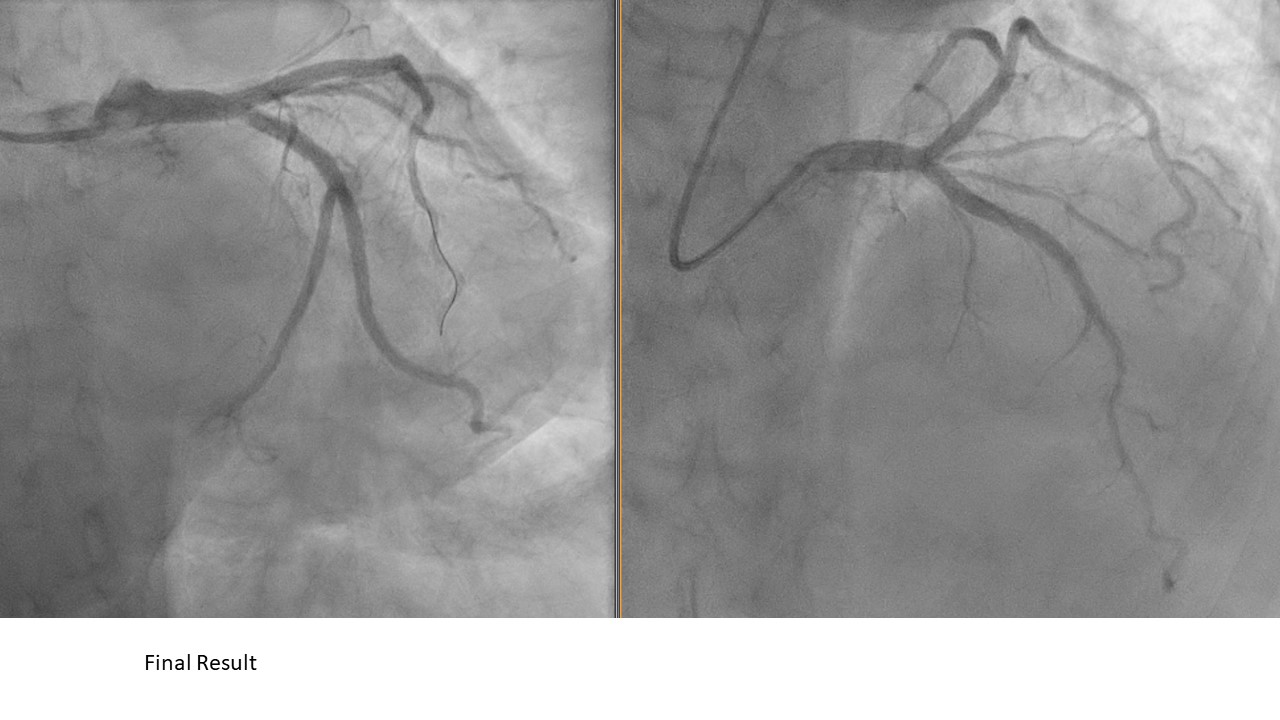
Guiding catheter EBU 3.5 6Fr was used to engage left coronary artery with good support, wired into LAD. Pre IVUS assessment revealed the minimal lumen area was 2.48mm2 at proximal LAD, 180 – 360 degree of superficial calcium from mid to proximal LAD, LAD size was 4mm and LM size was 6-7mm ( Fig. A, B, C). Rotablation to mid and proximal LAD with burr 1.75mm 5 runs at 180,000 rpm. Subsequently predilated LAD with NC balloon 3.0mm and scoring balloon 3.5mm.Stented mid to proximal LAD with DES 3.5 x 38mm and LM-LAD with 3.5x28mm (Synergy Megatron, Boston Scientific ). Post dilatation of LAD and LM with NC balloon 4.0. IVUS assessment post dilatation shown well opposed and good minimal stent area ( 13mm2 ) for LAD stent, however LM size was 7.0mm ,stent was undersize ( Fig. D ) , further upsize the LM stent with NC balloon 5.5x8mm and 6.0x8mm high pressure ( 20atm ). Good final PCI result . Patient was able to tolerate haemodialysis without chest pain , she was discharged well and medical therapy to RCA .
Case Summary
In our case, vascular access was a challenge for the patient . Distal left radial was used as she has right fistula and femoral puncture was avoided due to high aPTT post haemodialysis with heparin. The guiding catheter stability and support was good despite using the distal left radial access , able to perform rotablation with 1.75mm burr without difficulty. Another challenge in this case was size discrepancy in LAD and LM , an appropriate stent selection is important in order to upsize to desired stent size . Imaging in PCI is important especially for optimal stent sizing and enhanced lesion preparation e.g. atherectomy in our case.