
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-065
Severe Calcified Coronary Artery Disease, Aortic Stenosis and Cardiogenic Shock in an Elderly Man a 5-Step Multi-Disciplinary Solution
By Muhammad Andi Yassiin, Sofian Johar, Rajinikanth Rajagopal, Keyvan Kamalvand, Nadzir Juanda, Dhakshinamoorthi Periasamy
Presenter
Muhammad Andi Yassiin
Authors
Muhammad Andi Yassiin1, Sofian Johar2, Rajinikanth Rajagopal3, Keyvan Kamalvand3, Nadzir Juanda3, Dhakshinamoorthi Periasamy3
Affiliation
Jakarta Heart Center, Indonesia1, RIPAS Hospital, Brunei Darussalam2, Gleneagles JPMC, Brunei Darussalam3,
View Study Report
TCTAP C-065
CORONARY - Cardiac Surgery/Hybrid Revascularization
Severe Calcified Coronary Artery Disease, Aortic Stenosis and Cardiogenic Shock in an Elderly Man a 5-Step Multi-Disciplinary Solution
Muhammad Andi Yassiin1, Sofian Johar2, Rajinikanth Rajagopal3, Keyvan Kamalvand3, Nadzir Juanda3, Dhakshinamoorthi Periasamy3
Jakarta Heart Center, Indonesia1, RIPAS Hospital, Brunei Darussalam2, Gleneagles JPMC, Brunei Darussalam3,
Clinical Information
Patient initials or Identifier Number
AAH
Relevant Clinical History and Physical Exam
73 man, Known Severe AS, Late presentation Anterior STEMI, Failed PCI to LAD CTO, Severe LVSD.Planned surgery – high risk, VF arrest - Resuscitated, High inotropes, MDT discussion and family discussion, Cardiogenic shock , Prognosis guarded; high mortality risk, ECMO + PCI + TAVI
ECMO - Ultrasound guided, Left Common Femoral Artery – 17F, Left Femoral Vein – 23F, Antegrade flow – Superior femoral artery – 4F

 ROTA TAVI ECMO.jpg
ROTA TAVI ECMO.jpg
ECMO - Ultrasound guided, Left Common Femoral Artery – 17F, Left Femoral Vein – 23F, Antegrade flow – Superior femoral artery – 4F
Relevant Test Results Prior to Catheterization
ECG - SR, anterior ST elevation, lateral ST depression with inverted T waveEcho - Severe aortic stenosis. Severe LV dysfunction. LVEF 25% AVA 0.68cn2, MPG 30 mmHg, PPG 50 mmHg.MSCT - Shown in the picture
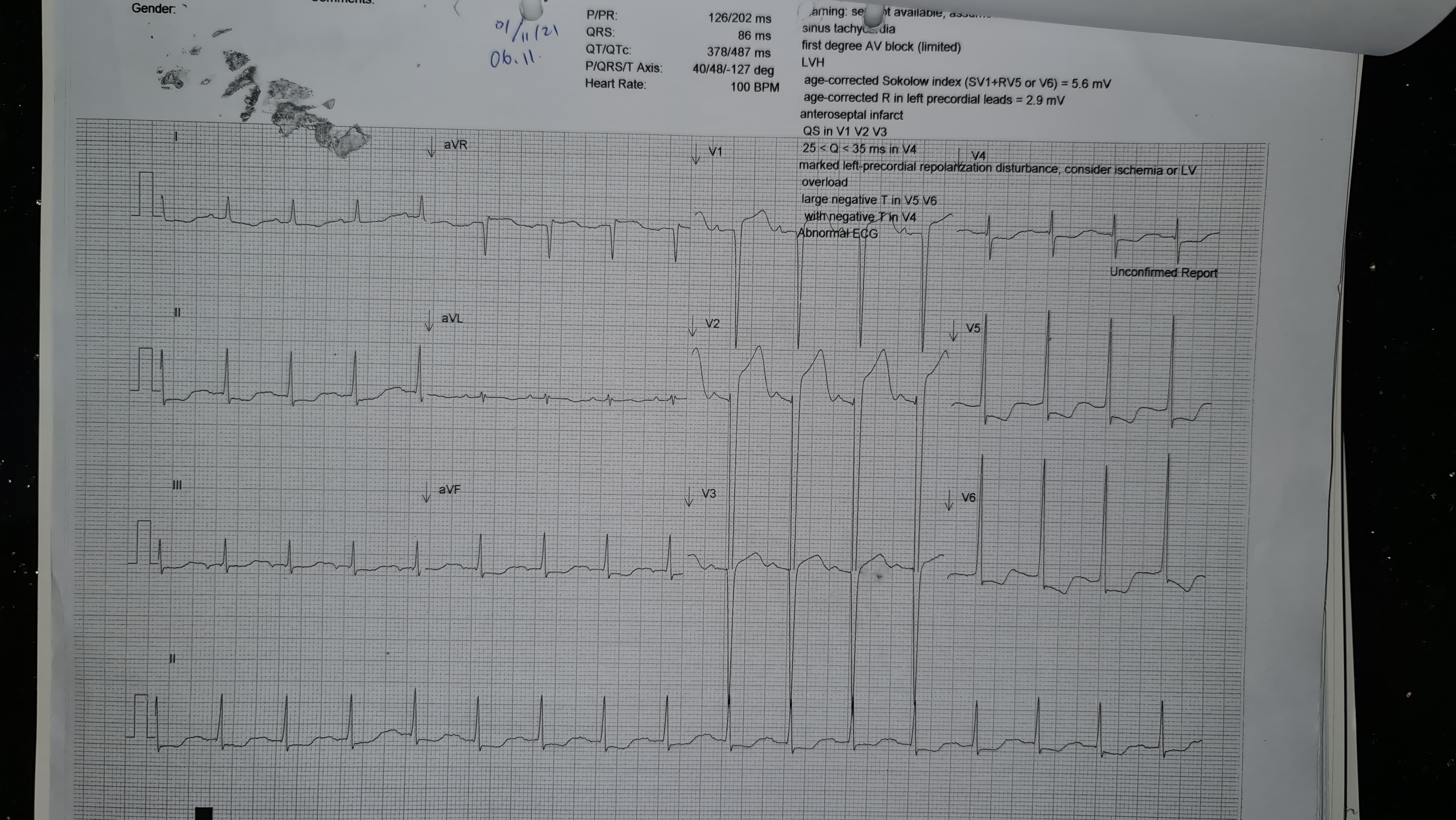
ROTA TAVI ECG.jpg
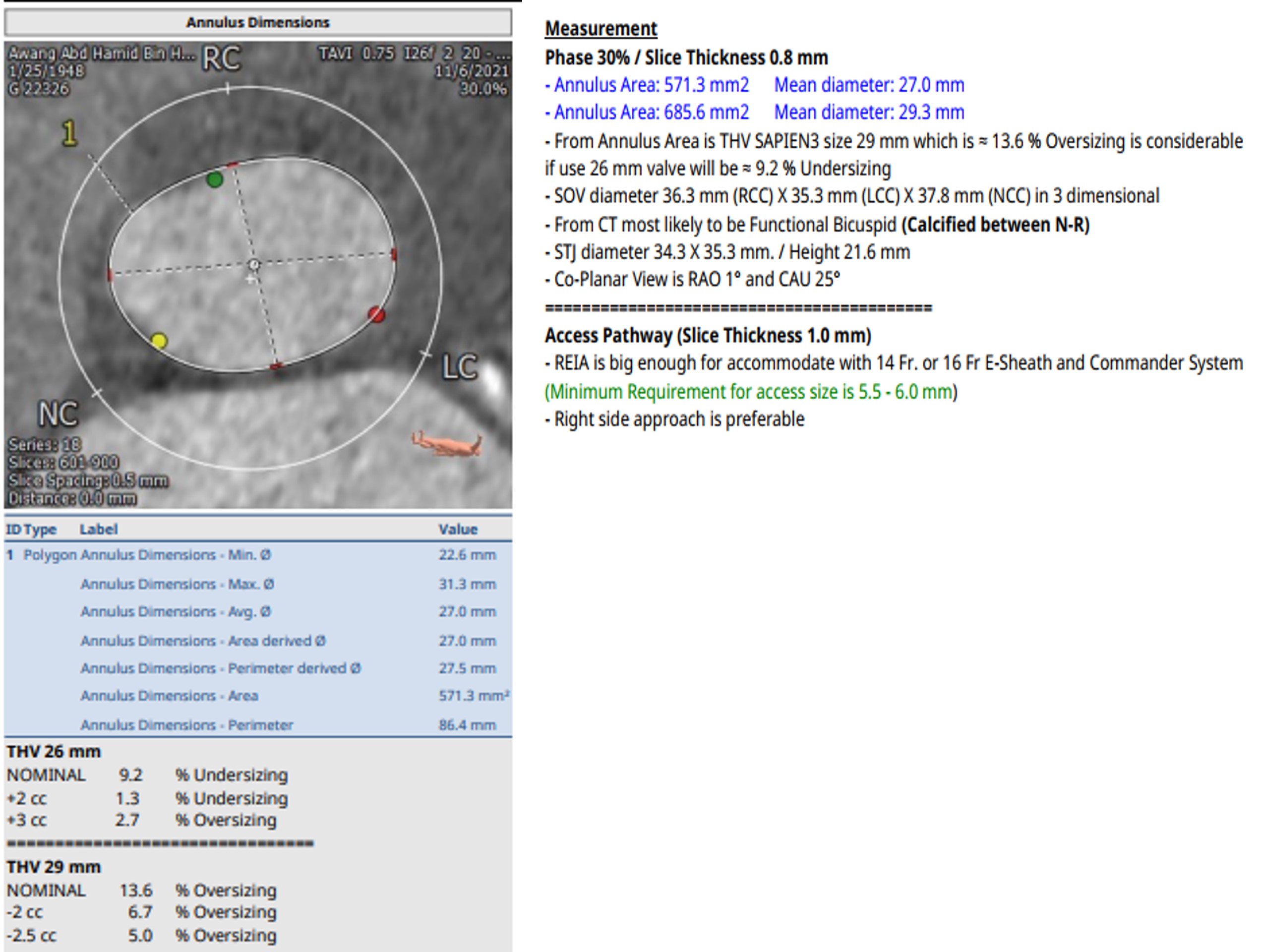
ROTA TAVI MSCT Measurement.jpg
Relevant Catheterization Findings
CAG - Moderate ostial LMS stenosis with 6F guide damping.LAD heavily calcified with severe disease throughout and CTO mid vessel with collaterals from RCANo severe stenosis in Cx/OMModerate mid RCA stenosis, significant PDA stenosis, collaterals to LAD
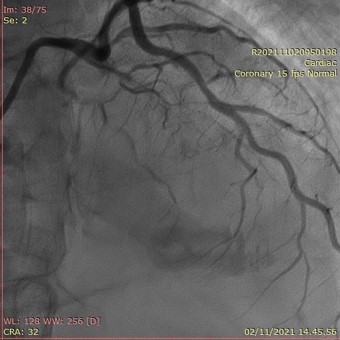
ROTA TAVI CAG LAD CTO.jpg
Interventional Management
Procedural Step
PCI to CTO LAD November 5th, 2021 - EBU 4 guide, Finecross placed in mid-LAD and Rota Floppy wire passed to dLAD. Rotablation with 1.5mm burr - 3 runs up to mid-LAD. IVUS - 180 degress calcium; LAD 3.5mm, LMS 4.5mm. Mid and proximal LAD pre-dilated with 2mm, 2.5mm Wolverine and 3mm NC balloons. Xience 2.75x23mm and 3.5x28mm DES placed from mid-LAD to ostial LMS. Post-dilated with 4.5mm NC balloon in LMS and 3.5mm NC balloon in LAD to high pressures. Guideliner delivered to dLAD. 2 mm NC balloon passed to dLAD, then Xience 2x28mm DES deployed at 9-16atm. Overlap post-dilated with 2.5mm NC balloon. Good result with BP improving from 90 systolic to 140 systolic after PCI.
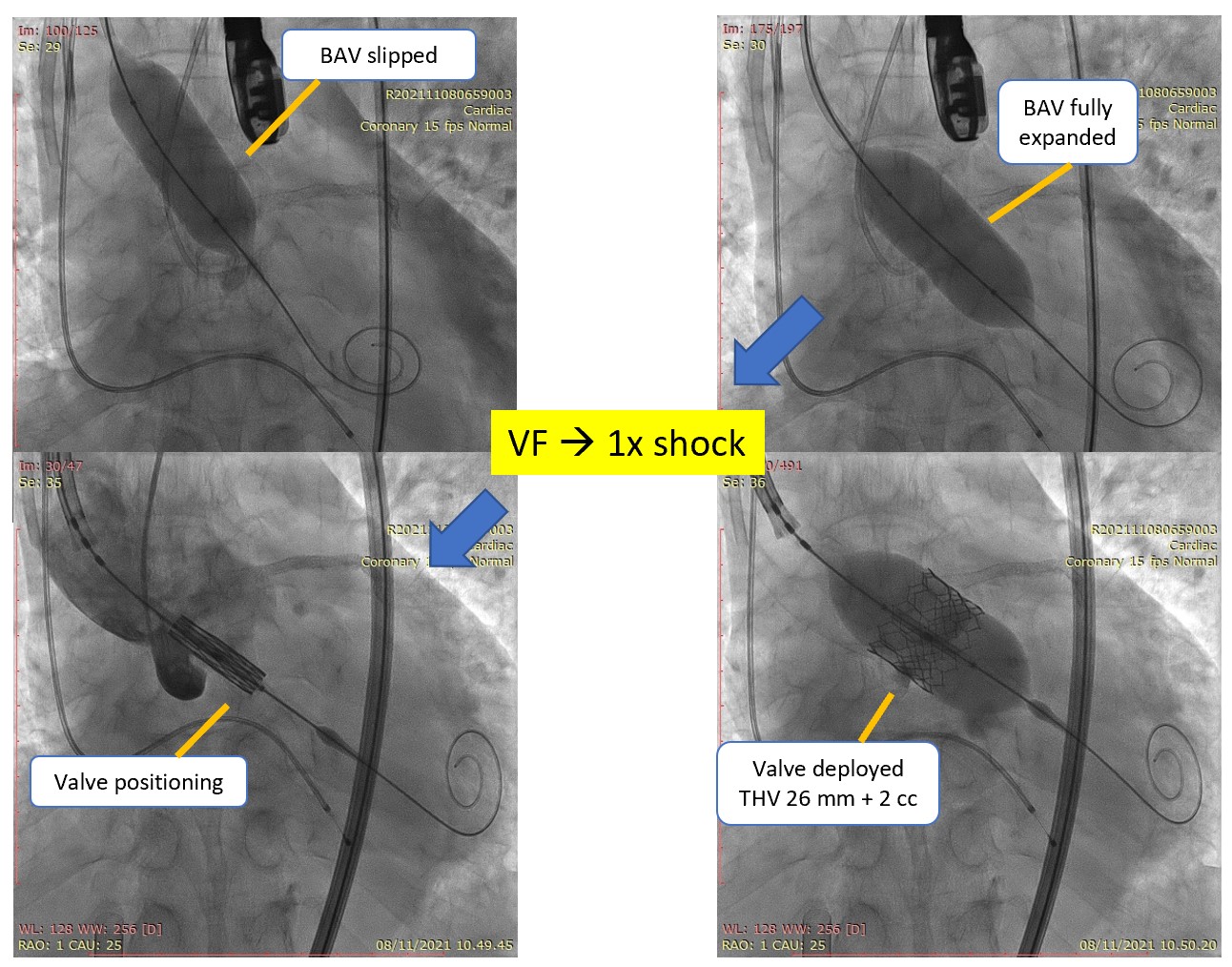
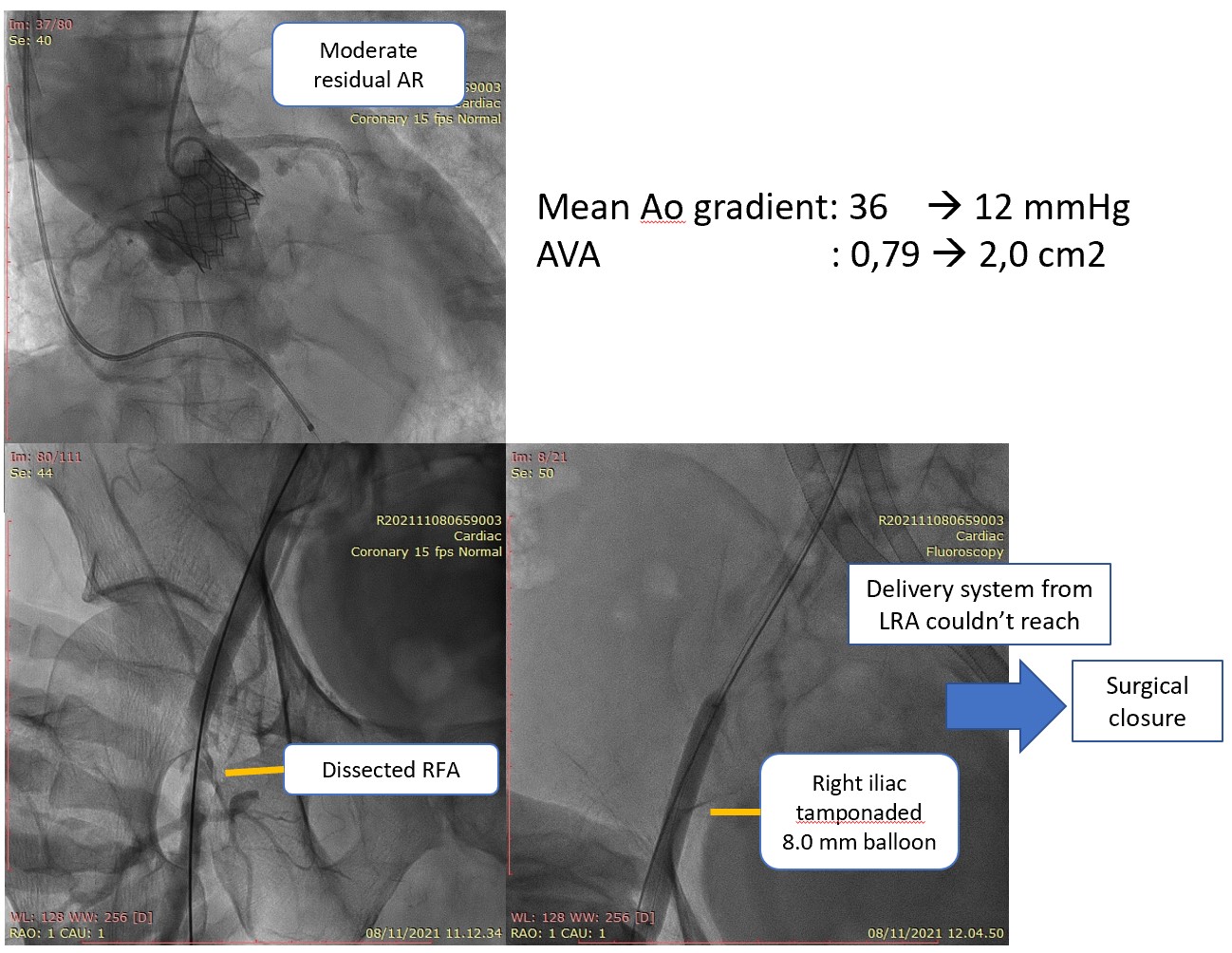
TAVI for Severe AS November 8th, 2021 - E sheath inserted over stiff wire, but unable to advance past a calcific shelf in the aorta. ECMO cannula pulled back and required pre-dilation with a 7.0 then 10.0 balloon to allow advancement of TAVI sheath. Aortic valve crossed with a AL2/straight wire then exchanged for pigtail. Calculated AVA 0.79 cm2, mean gradient 36 mmHg. Pre-dilated under rapid pacing with the 23mm balloon. 1 x VF requiring defibrillation, 1 further episode of VF which self-terminated just prior to shock delivery. Sapien 3 26mm valve with extra 2cc (total 25 cc in indeflator) deployed under rapid pacing with good result. Moderate residual AR, flow noted in LAD. Post-procedure mean gradient 12.3 mmHg and AVA 2.0cm2. Unable to deploy Proglide sutures in RFV - failed. Proceeded to operative repair.
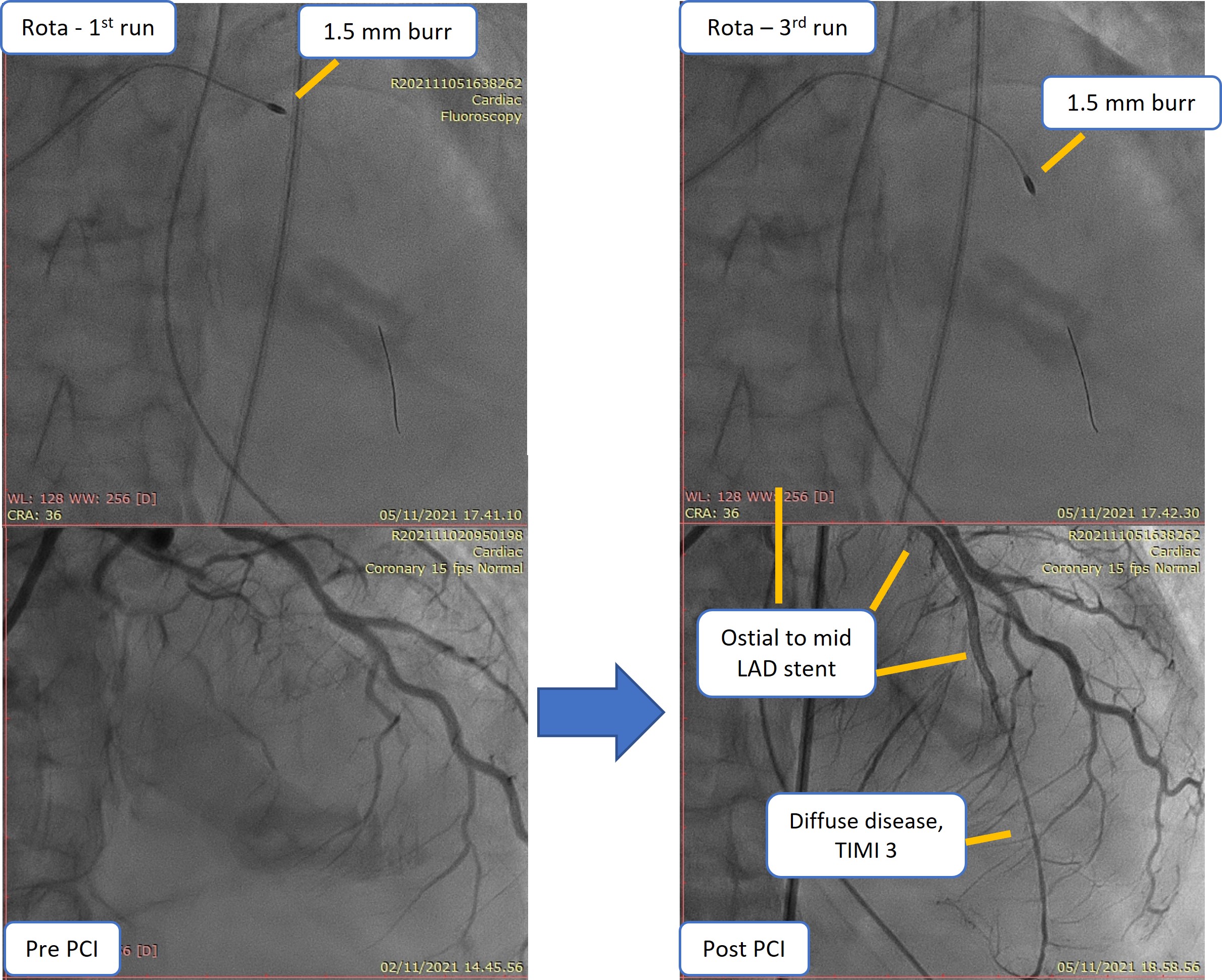
ROTA TAVI PCI Procedure.jpg
ROTA TAVI TAVI Procedure 2.jpg
ROTA TAVI TAVI Procedure 3.jpg
TAVI for Severe AS November 8th, 2021 - E sheath inserted over stiff wire, but unable to advance past a calcific shelf in the aorta. ECMO cannula pulled back and required pre-dilation with a 7.0 then 10.0 balloon to allow advancement of TAVI sheath. Aortic valve crossed with a AL2/straight wire then exchanged for pigtail. Calculated AVA 0.79 cm2, mean gradient 36 mmHg. Pre-dilated under rapid pacing with the 23mm balloon. 1 x VF requiring defibrillation, 1 further episode of VF which self-terminated just prior to shock delivery. Sapien 3 26mm valve with extra 2cc (total 25 cc in indeflator) deployed under rapid pacing with good result. Moderate residual AR, flow noted in LAD. Post-procedure mean gradient 12.3 mmHg and AVA 2.0cm2. Unable to deploy Proglide sutures in RFV - failed. Proceeded to operative repair.
Case Summary
In critically ill, post-arrest patient with high mortality – MDT (Multi-Discipline Team) is crucial for patient selection and management. ECMO provides full cardiopulmonary support during both PCI and TAVI procedure. Remote proctoring is very useful especially in this pandemic time