
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-029
Ostial LM STEMI
By Chun Lin Raymond Cheung
Presenter
Chun Lin Raymond Cheung
Authors
Chun Lin Raymond Cheung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1,
View Study Report
TCTAP C-029
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Ostial LM STEMI
Chun Lin Raymond Cheung1
Tuen Mun Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Mr Ho
Relevant Clinical History and Physical Exam
Mr Ho was a 73 year old retired driver, with smoking history of 60 pack years. He has a past health of hypertension and hyperlipidemiaHe complained of sudden onset of chest pain during fishing at 5pm, followed with shortness of breath On admission, BP 128/75 P 105 SpO2 95% 3L O2There is basal crepitation on auscultation and no ankle edema
ECG showed Sinus rhythm, HR 87bpm, ST elevation at AVR with diffuse ST depression V2-6, suggestive of Left Main STEMIPPCI was activated
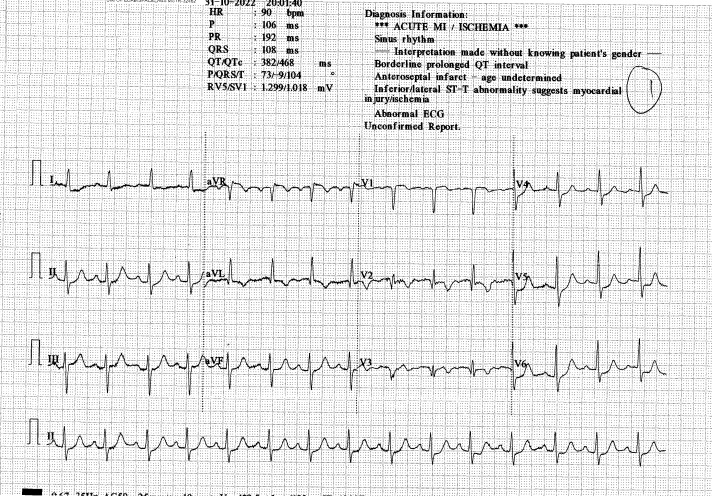
ECG showed Sinus rhythm, HR 87bpm, ST elevation at AVR with diffuse ST depression V2-6, suggestive of Left Main STEMIPPCI was activated
Relevant Test Results Prior to Catheterization
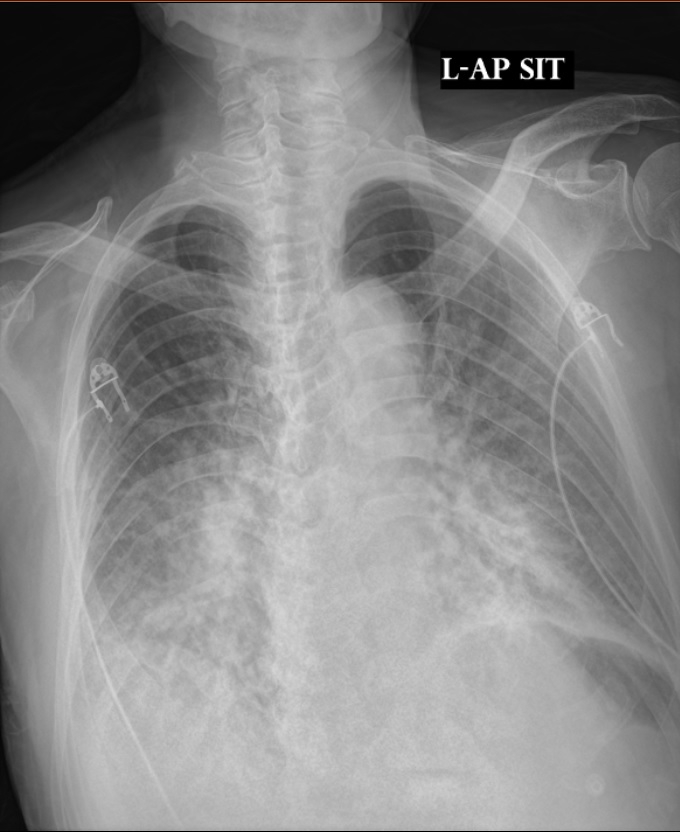
CXR congested.Complete blood count, liver and renal function tests were unremarkable.Cardiac markers were slightly elevated.
bedside V scan: normal LV size and systolic function, EF 55%, trileaflet calcified AV, mil AR, moderate functional MR, mild TR, no pericardial effusion
bedside V scan: normal LV size and systolic function, EF 55%, trileaflet calcified AV, mil AR, moderate functional MR, mild TR, no pericardial effusion
Relevant Catheterization Findings
LMS: oLM ATO, no damping RCA: dominant, mRCA minor disease, proximal PL branch 80-90% disease, retrograde supply to LAD, ostial PDA 90% diseaseConclusion: IRA = LM to LAD
 LMATO.avi
LMATO.avi
rca2.avi
rca.avi
Interventional Management
Procedural Step
LMS engaged with JL 3.5; RCA engaged with JR4 for contralateral injection Initially failed wiring LAD with different workhorse and CTO wires.
Proceeded to PCI to RCA firstRCA engaged with JR4, wired with NS runthrough til PL branch,PL branch dilated 2.0 balloon and stented with 2.5/15 Orsiro
Reattempt LAD wiring again with NS runthrough, Gaia next, fielder FC, fielder XTRIVUS guided wiring and crusade assisted wiring done, but still failed pLCx is likely CTO from wire feeling, decided not for further wiring Fielder FC directed to ramus first.LMS was dilated with 2.0 & 3.0 balloon with IVUS guidance Finally LMS til D1 was wired with sion black with special shape with crusade support IVUS showed diffuse disease from oLM til pLAD and confirmed entry to true lumen
Crusade was exchanged to sion black wireFielder XT R was used to redirect to LADA dissection flap over pLAD was suspectedGentle movement of the XT -R crossed the lesion and entered D2Crusade was exchanged to XT RRunTh cannot redirect into LADSion black with special shape was used again and entered dLAD, confirmed by wire feel and angiogram
LMS -pLAD was then dilated with 2.0 and 3.0 balloon, mLAD was dilated with 2.75 balloon mLAD stented with orsiro 2.25/40LM-pLAD stented with Orsiro 3.5/40 LM stent post dilated with 4.0 balloon, pLAD stent post dilated with 3.25 balloon Final angio showed TIMI III flow and nil acute complication
Successful IVUS guided PTCA/S to PL with DES x1 & oLM-mLAD with DES x2
wireramus.avi
wireddiagonal.avi
finalshot.avi
Proceeded to PCI to RCA firstRCA engaged with JR4, wired with NS runthrough til PL branch,PL branch dilated 2.0 balloon and stented with 2.5/15 Orsiro
Reattempt LAD wiring again with NS runthrough, Gaia next, fielder FC, fielder XTRIVUS guided wiring and crusade assisted wiring done, but still failed pLCx is likely CTO from wire feeling, decided not for further wiring Fielder FC directed to ramus first.LMS was dilated with 2.0 & 3.0 balloon with IVUS guidance Finally LMS til D1 was wired with sion black with special shape with crusade support IVUS showed diffuse disease from oLM til pLAD and confirmed entry to true lumen
Crusade was exchanged to sion black wireFielder XT R was used to redirect to LADA dissection flap over pLAD was suspectedGentle movement of the XT -R crossed the lesion and entered D2Crusade was exchanged to XT RRunTh cannot redirect into LADSion black with special shape was used again and entered dLAD, confirmed by wire feel and angiogram
LMS -pLAD was then dilated with 2.0 and 3.0 balloon, mLAD was dilated with 2.75 balloon mLAD stented with orsiro 2.25/40LM-pLAD stented with Orsiro 3.5/40 LM stent post dilated with 4.0 balloon, pLAD stent post dilated with 3.25 balloon Final angio showed TIMI III flow and nil acute complication
Successful IVUS guided PTCA/S to PL with DES x1 & oLM-mLAD with DES x2
Case Summary
This case highlights a difficult situation with complex lesion difficult to cross in acute condition. Initially different workhorse and CTO wires have failed to cross the lesion with microcatheter support. Subsequently the patient was deteriorating on table with desaturation. Action had to be taken to quickly stabilize the patient. Strategy has switched to PCI to RCA first to improve flow to LAD. Ramus was wired first to provide support for LMS predilatation to allow successful wiring of LAD afterwards. This shows that strategy and plan would have to be modified quickly depending on clinical situation in complex cases.