
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-089
High Risk Percutaneous Coronary Intervention in Old Age, LCx CTO and LM Bifurcation Lesion - How We Succeeded
By Yuan-Hung Wang, Yen-Lien Chou
Presenter
Yuan-Hung Wang
Authors
Yuan-Hung Wang1, Yen-Lien Chou1
Affiliation
Tri-Service General Hospital, Taiwan1,
View Study Report
TCTAP C-089
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
High Risk Percutaneous Coronary Intervention in Old Age, LCx CTO and LM Bifurcation Lesion - How We Succeeded
Yuan-Hung Wang1, Yen-Lien Chou1
Tri-Service General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
2003166
Relevant Clinical History and Physical Exam
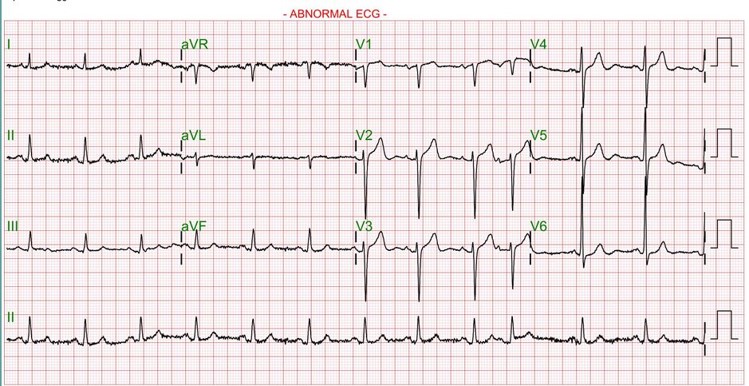
Chest tightness and dyspnea on exertion recentlyHistory : Hypertension and hyperlipidemia without regular medicationsECG : Sinus rhythm and atrial premature contractionPhysical exam:No basal ralesNo peripheral edema
Relevant Test Results Prior to Catheterization
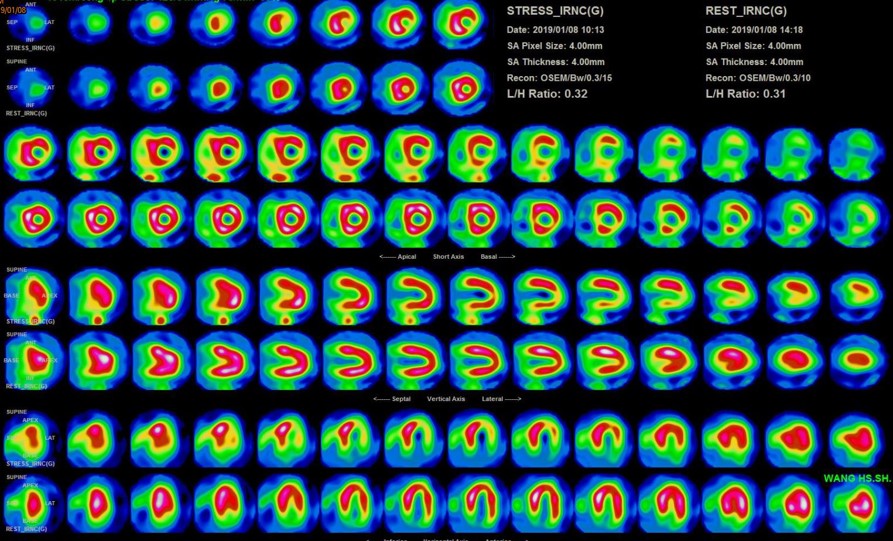
Tl-201 myocardial perfusion scan : Myocardial ischemia over 55% LCX territory in pharmacologic stress
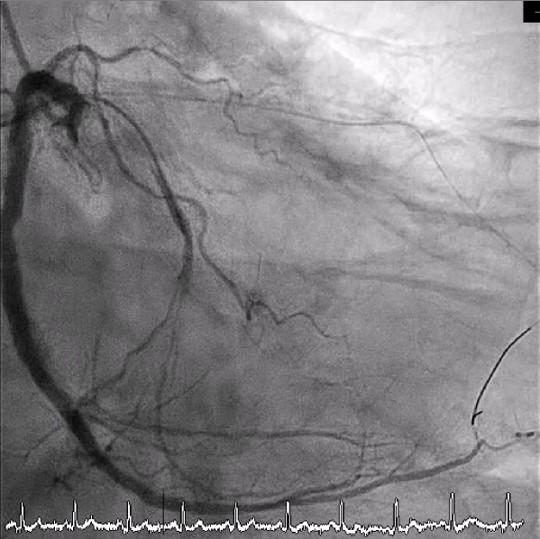
Relevant Catheterization Findings
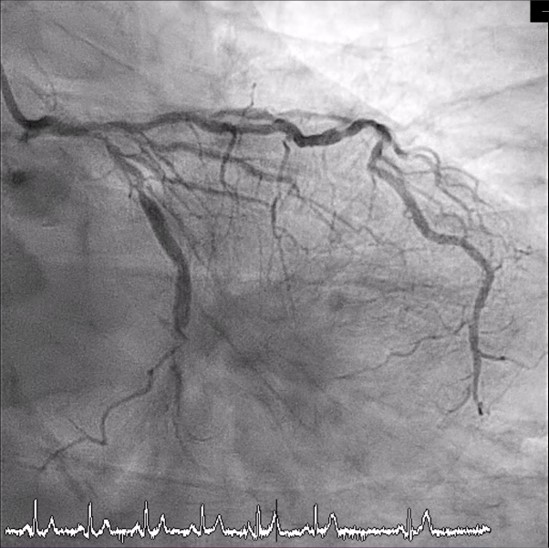
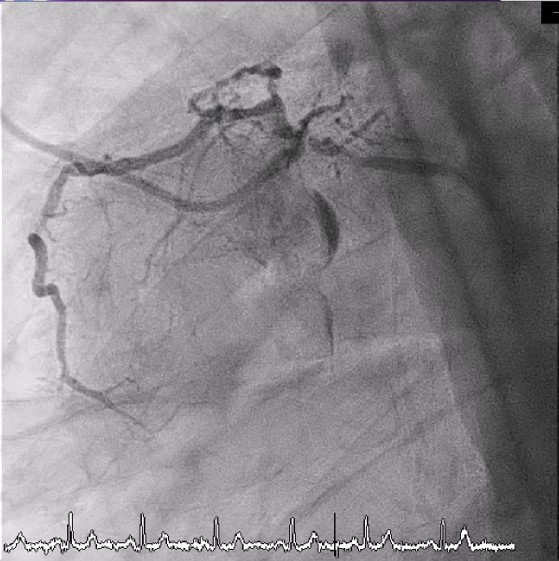
LMCA : - M/3 : Tubular stenosis, max 70-80 % ; Medina (1,1,1)LAD : Luminal irregularity (LI)- P/3 : Segmental stenosis, max 80 %- M/3 : Segmental stenosis, max 80 %LCx : LI, severe calcification, and tortuous vessel- P/3: Segmental stenosis, max 90 %- M/3 : Chronic total occlusion (CTO)- Ostium of OM1 : CTORCA : LI and calcification- P/3 to D/3 : Diffuse stenosis, max 90 %- Ostium to P/3 of PL : Segmental stenosis, max 90 %- P/3 to M/3 of PDA : Tubular stenosis, max 80 %

Interventional Management
Procedural Step
1st CAG
1. Balloon dilation and stent implantation over os-RCA to p-PL.
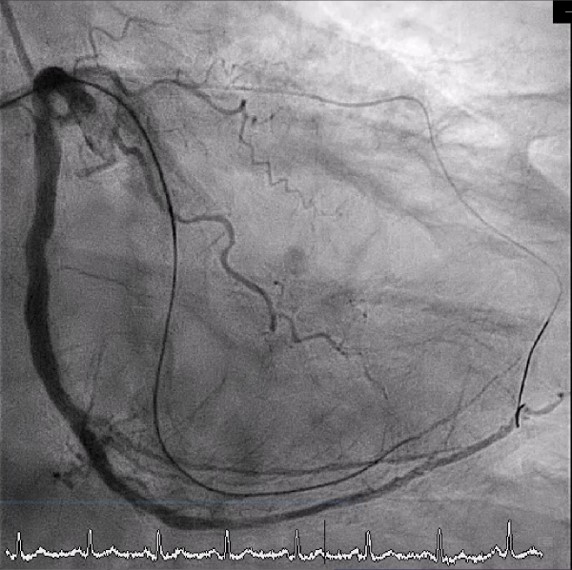
2nd CAG
1. SION wire was advanced to d-LAD and SION blue wire was advanced to m-LCX before CTO lesion.
2. Balloon dilation over m-LM to m-LAD and m-LM to m-LCX.
3. Corsair microcatheter was along SION Blue wire to m-LCX.
4. Antegrade approach with XTR wire was successfully penetrated the CTO cap over m-LCX after wire escalation, and the XTR wire was advanced to d-LCX, which
was confirmed at true lumen by angiography from RCA ostium
5. Balloon dilation and stent implantation from LM to LAD & LCX were performed. No residual stenosis or thrombus, also with no other complication.
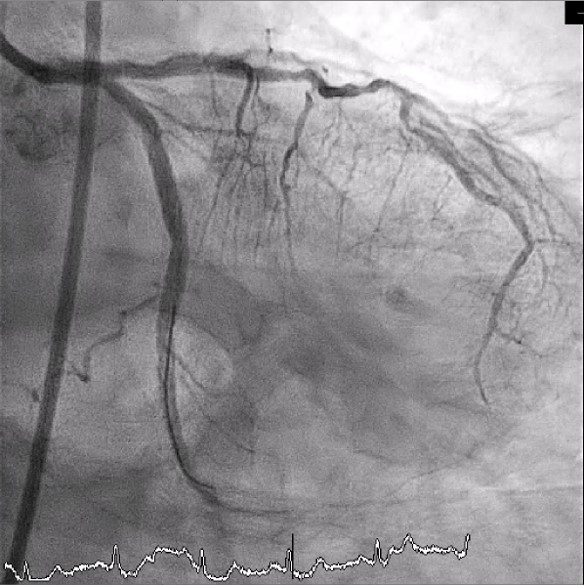
Case Summary
1. CTO PCI by using “ Hybrid Approach” appears efficient.2. Good angiography by dual injections is fundamental for CTO PCI.3. CTO lesion characteristics non-ambiguous proximal cap suitable for antegrade approach should be clarified.4. Changes in crossing strategy are based on angiographic characteristics of the CTO.