
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-099
Double Trouble ! Coronary Dissection by Balloon Rupture Followed by Stuck IVUS After Stenting in a Rotational Atherectomy Case
By Wei-Cheng Chang
Presenter
Wei-Cheng Chang
Authors
Wei-Cheng Chang1
Affiliation
Tri-Service General Hospital, Songshan Branch, Taiwan1,
View Study Report
TCTAP C-099
CORONARY - Complications (Coronary)
Double Trouble ! Coronary Dissection by Balloon Rupture Followed by Stuck IVUS After Stenting in a Rotational Atherectomy Case
Wei-Cheng Chang1
Tri-Service General Hospital, Songshan Branch, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Chen
Relevant Clinical History and Physical Exam
A 67 y/o woman, non-smoker, has history of diabetes, hypertension, hyperlipidemia. She had stented a DES at RCA one year ago due to unstable angina. In recent months, she presented with recurrent angina even with optimal medication. Physical examination revealed grade II systolic murmur at apex and lower left sternal border.
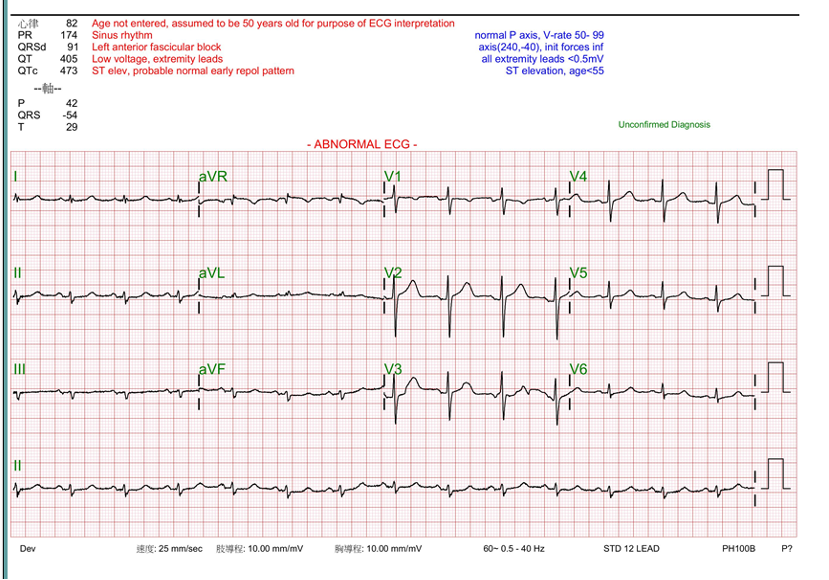
Relevant Test Results Prior to Catheterization
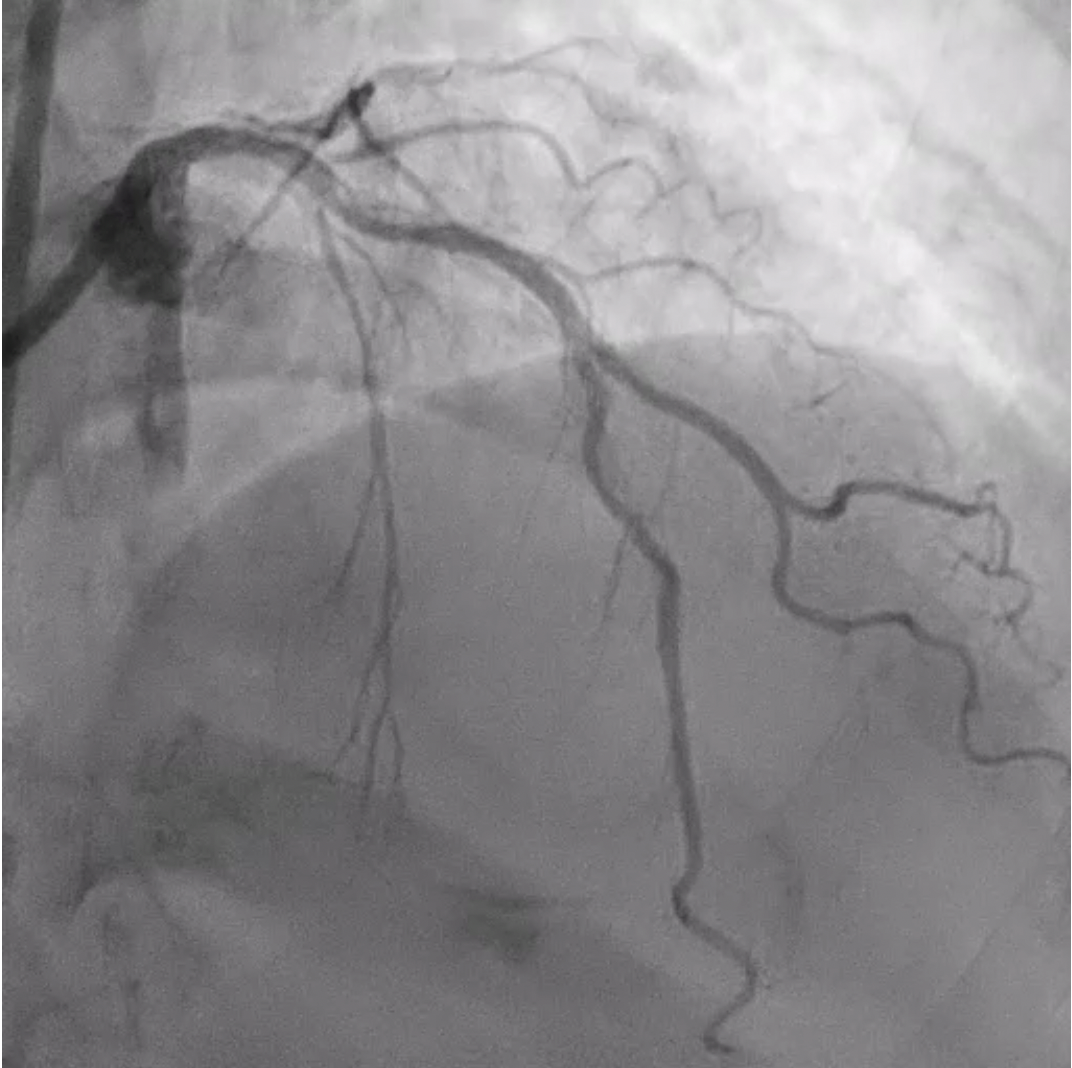
Relevant Catheterization Findings
LMCA: atherosclerosis
Interventional Management
Procedural Step
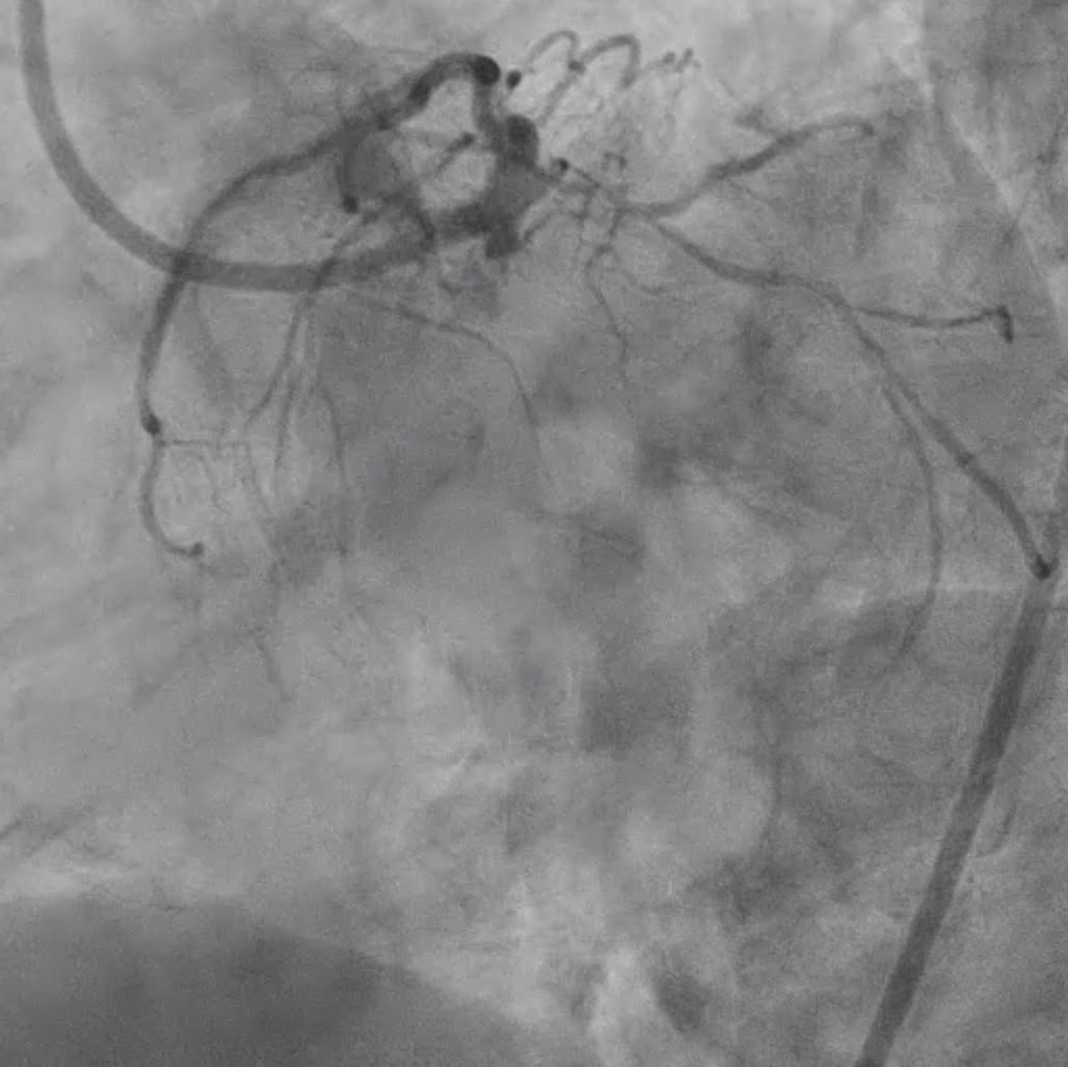
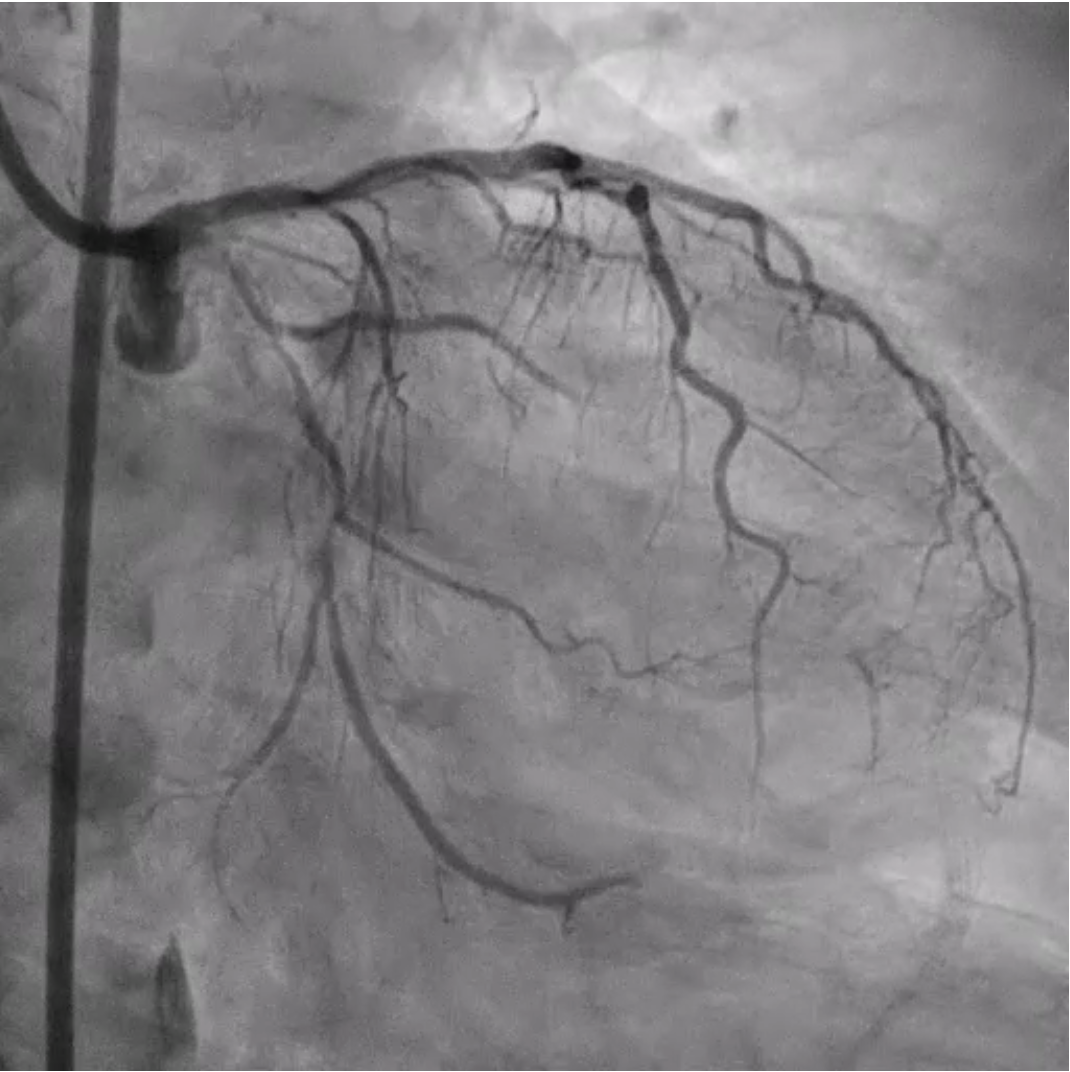
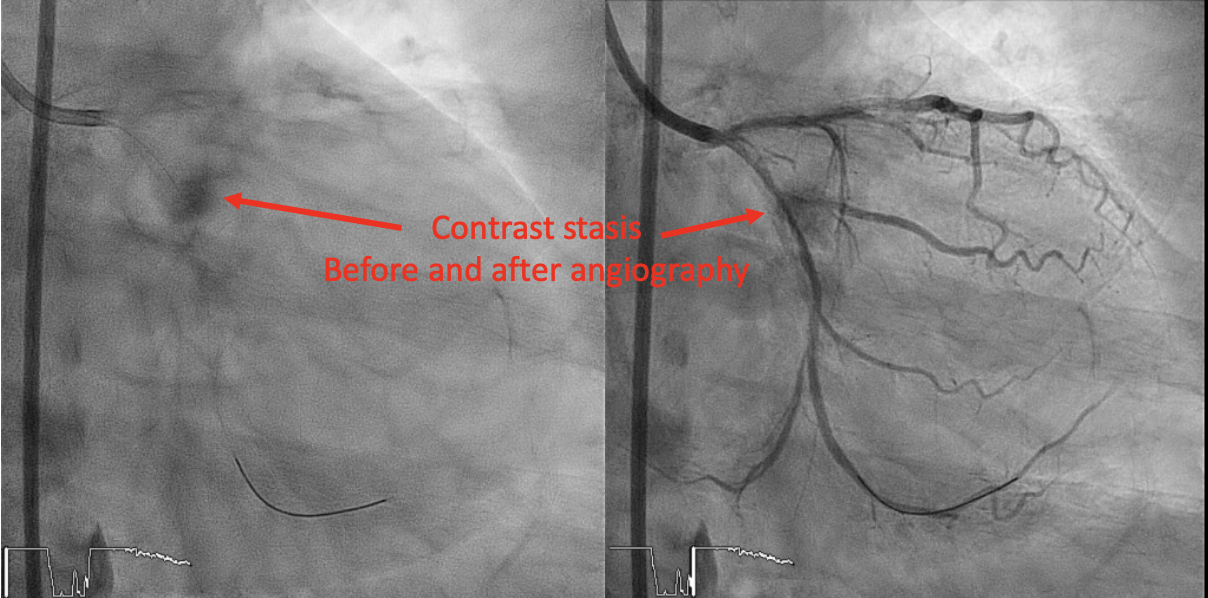
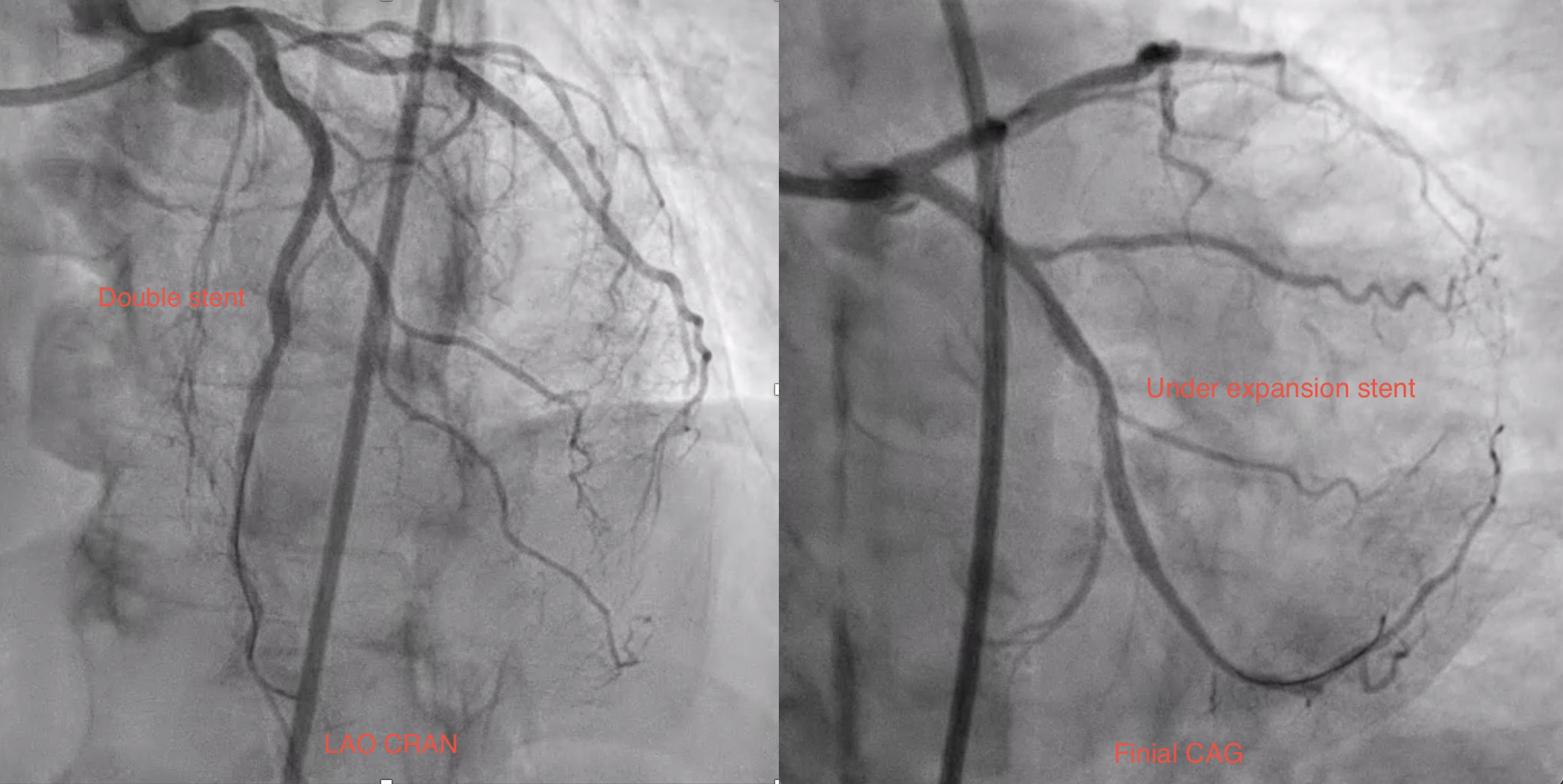
Used right femoral artery approach with EBU 3.0 7 F (side hole), SION wire to d-LCX, dilated by 2.0 x 15 mm balloon (un-dilatable). Rotational atherectomy done by 1.25 mm burr ( 100,000~120,000 rpm) for 3 times with Rota extrasupport wire. P-LCX lesion was dilated by 2.25 x 15 mm NC balloon, but m-LCX still presented an un-dilatable lesion. Increased the balloon pressure to 26 atm but it ruptured and causing coronary dissection. IVUS showed a p-LCX dissection at the m-LCX. Stented a 2.5 x 48 mm DES at p~m-LCX. Post-dilation by 2.5 x 12 mm NC balloon but m-LCX stent still not fully expand, however, TIMI 3 flow presented.
Case Summary
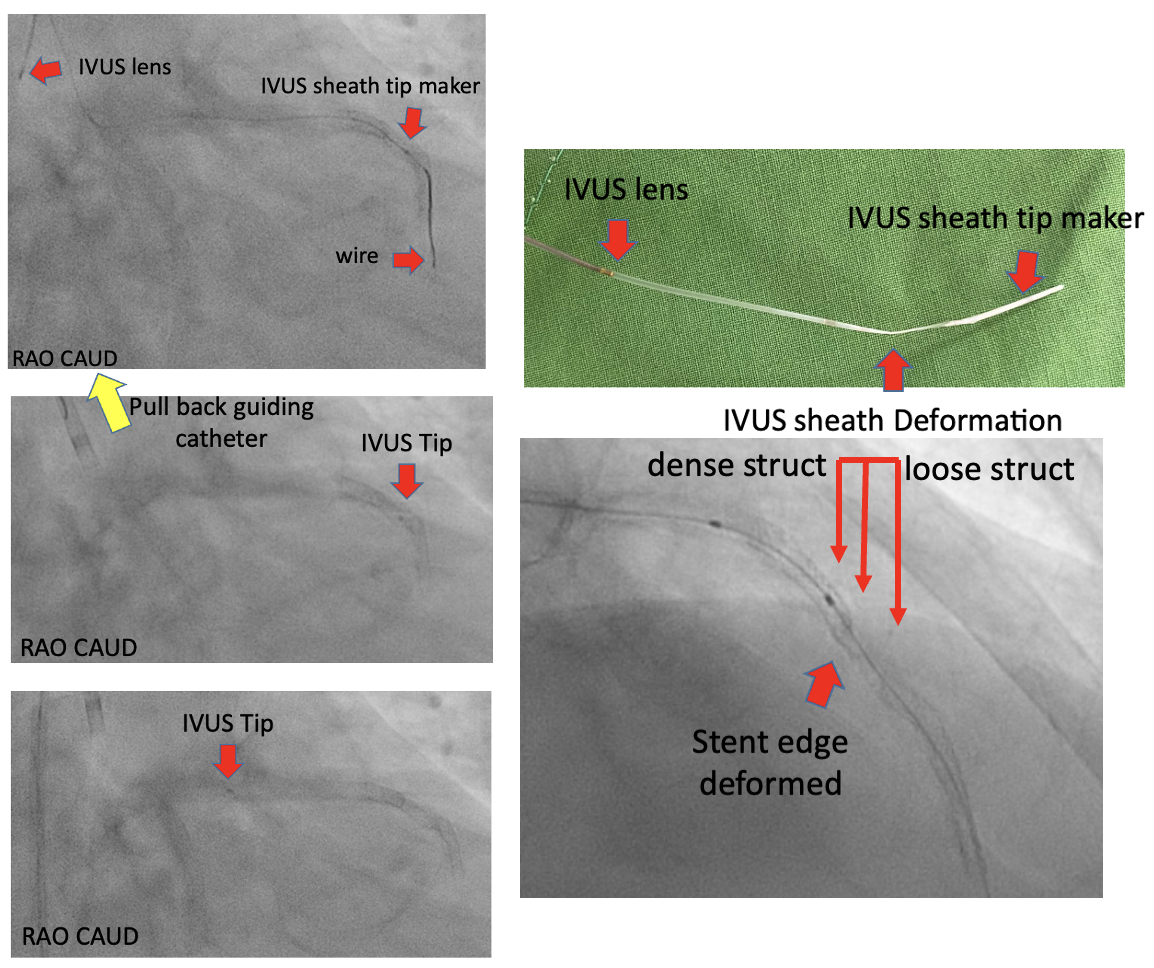
An NC balloon rupture caused by high pressure resulted in coronary dissection, which was treated with stenting.There was a risk that the IVUS sheath would stuck by stent especially before adequate post dilation. To pull the IVUS back, we withdraw the IVUS catheter, wire, and guiding catheter together. However, the step causing the longitudinal deformation of the stent. After wiring to true lumen, we placed another stent overlapping the reformatted stent. Perhaps there was another better way to resolve the stuck IVUS, such as wiring another wire, and inflating a balloon at the stuck spot.