
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-178
COVID-19 and Spontaneous Coronary Artery Dissection: Association or Causality
By Akshat Khurana
Presenter
Akshat Khurana
Authors
Akshat Khurana1
Affiliation
Christchurch hospital, New Zealand1,
View Study Report
TCTAP C-178
OTHERS - Women’s Health Issues
COVID-19 and Spontaneous Coronary Artery Dissection: Association or Causality
Akshat Khurana1
Christchurch hospital, New Zealand1,
Clinical Information
Patient initials or Identifier Number
JS
Relevant Clinical History and Physical Exam
A 55-year old woman was brought to emergency department complaining of sudden onset squeezing chest pain radiating to her arm and jaw and associated with giddiness. She had flu like illness a day prior to her presentation associated with malaise, arthralgia and dry cough. She had history of hypertension.Physical examination revealed dual heart sounds and clear lung fields to auscultation.
Relevant Test Results Prior to Catheterization
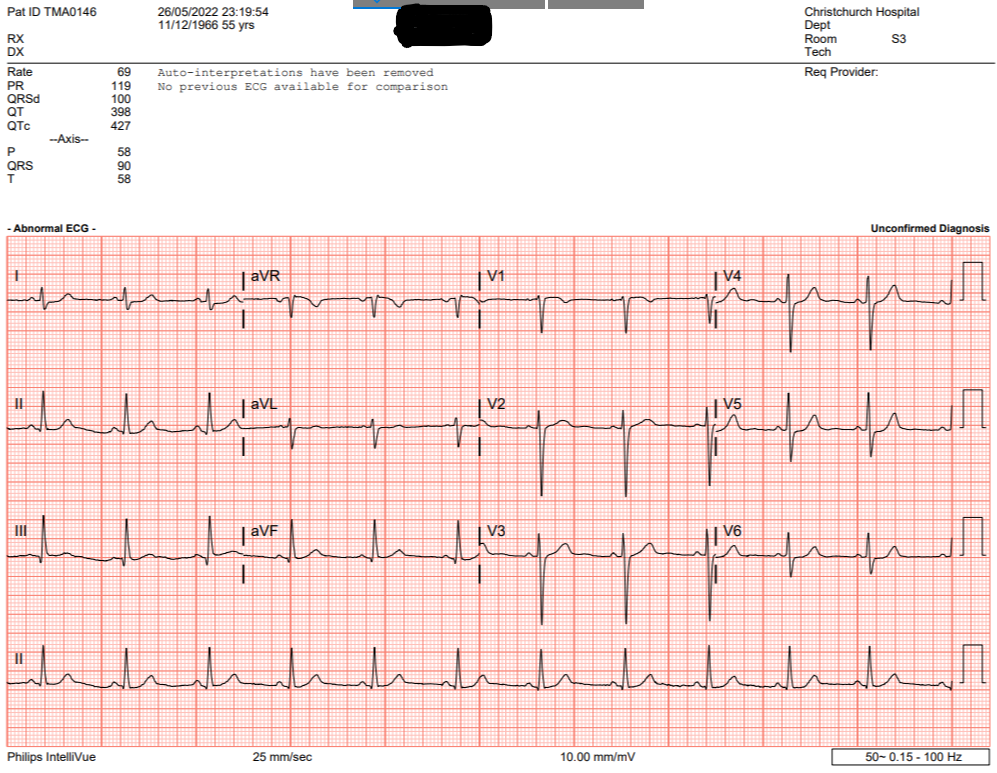
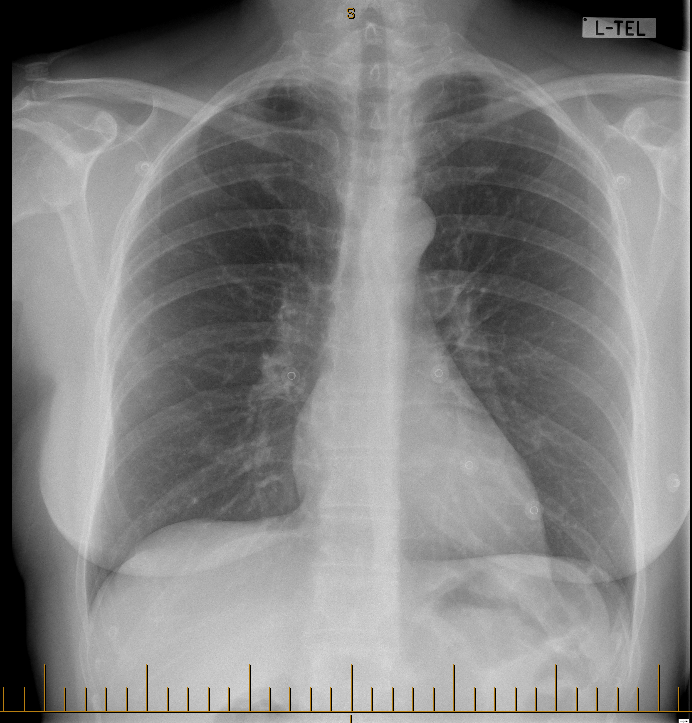
Electrocardiogram (ECG) showed normal sinus rhythm and thecardiac enzymes were elevated; high sensitivity troponin-I , 23000 ng/L (range0-10 ng/L). RNA PCR was positive for SARS-CoV-2 (COVID-19). D-Dimer was 303microgram/L (normal <500). Transthoracic echocardiogram showed severehypokinesis of the mid inferolateral wall with left ventricular ejectionfraction (LVEF) 52%. Chest X-ray showed no focal consolidation.
Relevant Catheterization Findings
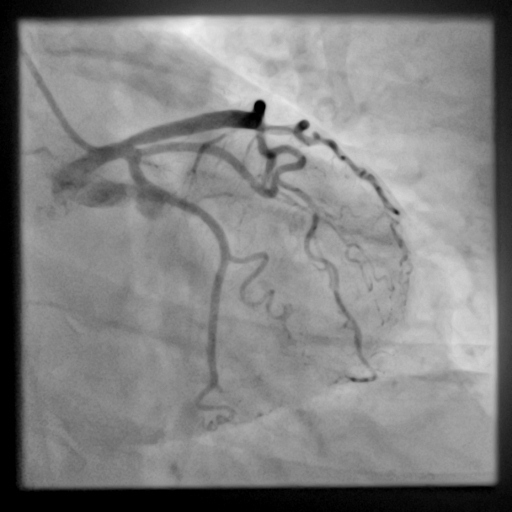
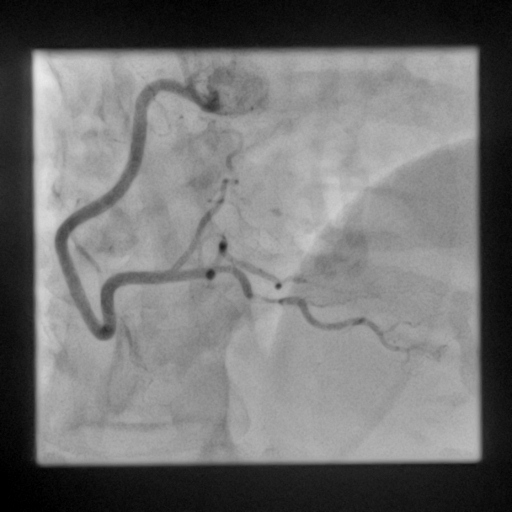
Invasive coronary angiogram showed tortuous coronary arteries with abrupt narrowing of mid- distal Ramus Intermiedius and discrete lesion of mid PDA. SCAD (spontaneous Coronary dissection) of Ramus Intermedius and mid PDA (posterior descending artery) was suspected and patient was treated conservatively. Repeat coronary angiography, few months later showed complete resolution of SCAD with normal appearance of affected vessels.

Interventional Management
Procedural Step
After obtaining an informed consent right Radial access was achieved with 6F Terumo sheath using over the wire technique. 1% lignocaine was used as local anaesthetic. 5F JL 3.5 (Judkin's) and JR 4 catheters were used to engage left main stem (LMS) and right coronary artery (RCA) and selective coronary angiography was performed. No percutaneous coronary intervention was performed. After the procedure hemoband (TR band) was applied to access site. Patient remained hemodyanamically stable throughout the procedure.



Case Summary
SCAD is a potential cause of type II myocardial infarction in patients with COVID-19, but more studies are needed to establish causality. Infection-related SCAD may occur at any time during index events and could be difficult to diagnose. Conservative management seems like a safe strategy.