
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-009
A Rare Case of Anterior Wall ST-Elevation Myocardial Infarction in a 28-Year Old, Male With a Solitary Coronary Artery Ostium
By Marie Sigourney Singidas Machacon-Wong, Marlou Ilagan Mendoza
Presenter
Marie Sigourney Singidas Machacon-Wong
Authors
Marie Sigourney Singidas Machacon-Wong1, Marlou Ilagan Mendoza1
Affiliation
Philippine Heart Center, Philippines1,
View Study Report
TCTAP C-009
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
A Rare Case of Anterior Wall ST-Elevation Myocardial Infarction in a 28-Year Old, Male With a Solitary Coronary Artery Ostium
Marie Sigourney Singidas Machacon-Wong1, Marlou Ilagan Mendoza1
Philippine Heart Center, Philippines1,
Clinical Information
Patient initials or Identifier Number
N. S. P.
Relevant Clinical History and Physical Exam
This is a case of a 28-year old male, obese, 10-pack year smoker, heavy alcoholic, marijuana user, with a family history of premature coronary artery disease, who came in for chest pain. He was diagnosed with ACS-STEMI in another institution where ACS regimen was loaded. He was then transferred to our institution for revascularization. At the ER, he was seen chest pain free with BP of 150/90 mmHg and heart rate of 93 beats/min. The rest of the physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
ECG revealed sinus rhythm, normal axis, recent anterolateral wall ST segment elevation myocardial infarction.
Relevant Catheterization Findings
(A) RAO cranial view showing a good-sized LAD with 99% mid segment stenosis after D1. (B) LAO caudal view showing an aortic injection revealing a blunt right and noncoronary sinuses without coronary origin. (C) RAO cranial view showing a large, dominant LCX extending to the atrioventricular groove supplying the RCA domain

Interventional Management
Procedural Step
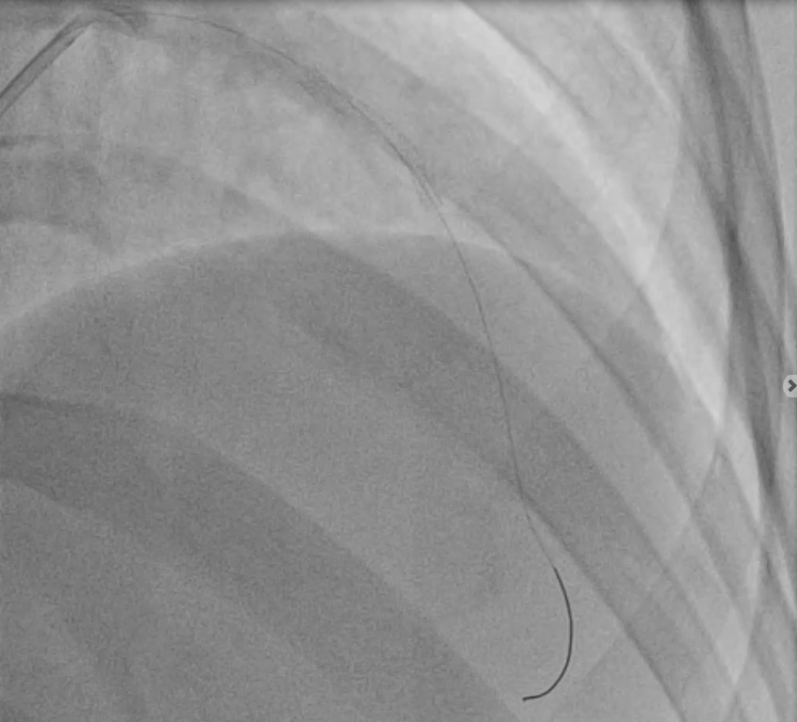
IVUS-guided percutaneous coronary intervention of the left anterior descending coronary artery was then done via the right transfemoral access. Intravenous heparin of 8500 units was given intraprocedurally. A 2.0 x 20 mm balloon was used to predilate the lesion. (Figure A) A 3.5 x 28 mm drug-eluting stent was then deployed from proximal to mid LAD. (Figure B) Post dilatation of the stent was done with a 3.5 x 12 mm balloon. (Video A and Figure C) Final angiography revealed a patent stent with TIMI 3 flow and no residual stenosis.


Case Summary
We report a case of an anterior wall ST-segment elevation myocardial infarction in a very young, male, obese patient with a solitary coronary artery ostium who is a heavy smoker, heavy alcoholic, marijuana user and with a family history of premature coronary artery disease. Coronary angiography accurately detected a 99% mid segment stenosis on the LAD artery and diagnosed a rare coronary artery anomaly. PCI of the occluded LAD was successfully done.