
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-164
"The Bermuda Triangle" - The OCT Contrast Swirl in the Left Main Stem That Kept Everyone Wondering
By Mugilan Sundarajoo, Hafidz Abd Hadi, Goay Swee En
Presenter
Mugilan Sundarajoo
Authors
Mugilan Sundarajoo1, Hafidz Abd Hadi2, Goay Swee En2
Affiliation
National Heart Institute Ijn, Malaysia1, National Heart Institute, Malaysia2,
View Study Report
TCTAP C-164
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular
"The Bermuda Triangle" - The OCT Contrast Swirl in the Left Main Stem That Kept Everyone Wondering
Mugilan Sundarajoo1, Hafidz Abd Hadi2, Goay Swee En2
National Heart Institute Ijn, Malaysia1, National Heart Institute, Malaysia2,
Clinical Information
Patient initials or Identifier Number
456456
Relevant Clinical History and Physical Exam
57 years old gentleman with Type 2 diabetes mellitus, hypertension and dyslipidemia presented with typical angina. He was treated as Non-ST Elevation Myocardial Infarction. Physical examination is unremarkable.
Relevant Test Results Prior to Catheterization
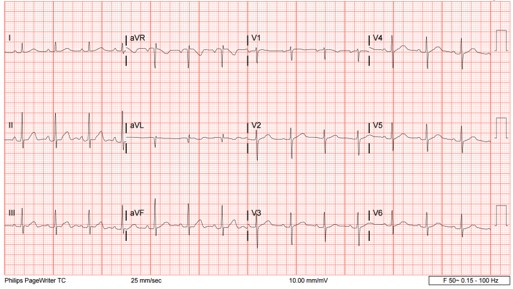
Troponin I upon presentation is 828ng/ml. ECG is sinus rhythm. Echocardiography reveals LV-EF of 59%.
Relevant Catheterization Findings
Right radial approach
LMS: mild disease (20-30% stenosis)

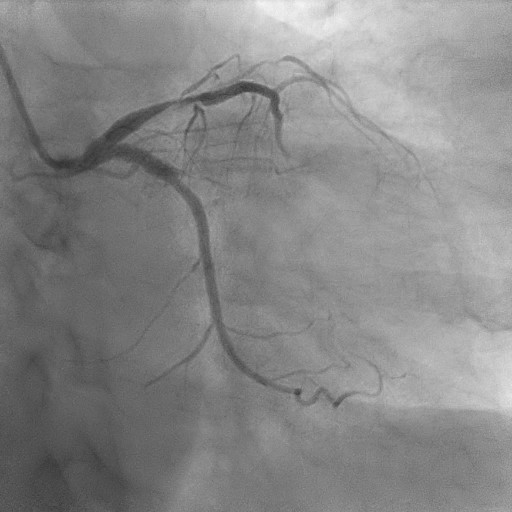
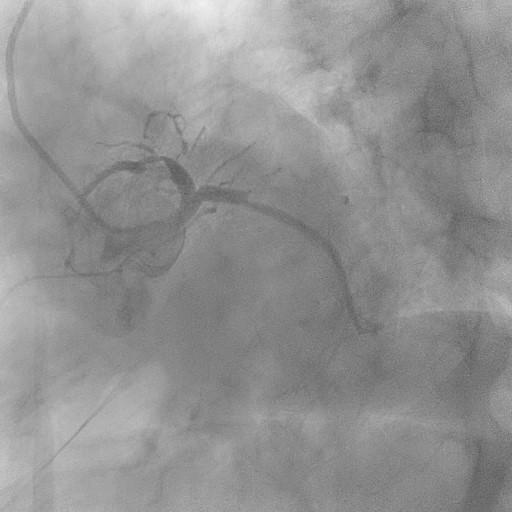
LMS: mild disease (20-30% stenosis)
Interventional Management
Procedural Step
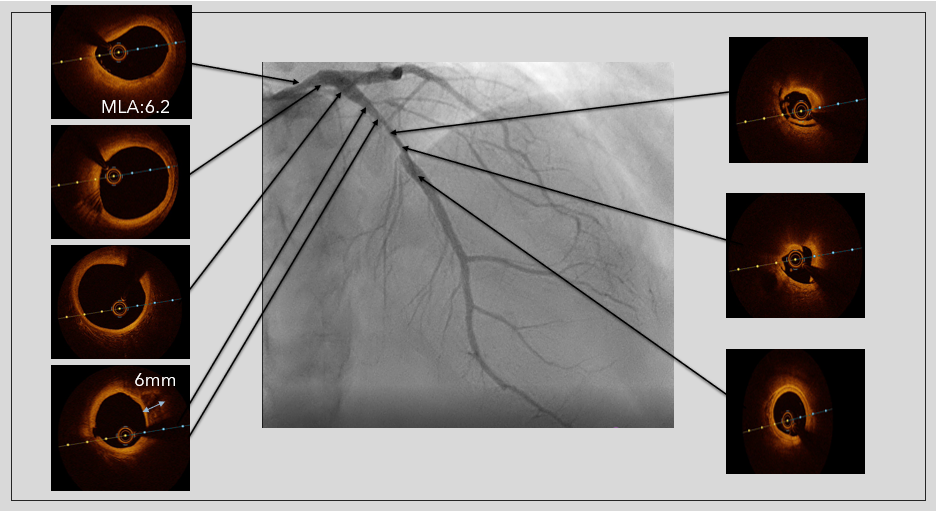
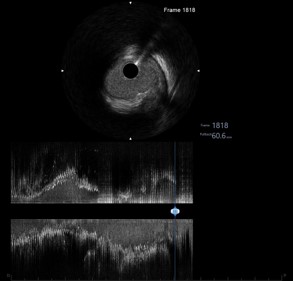
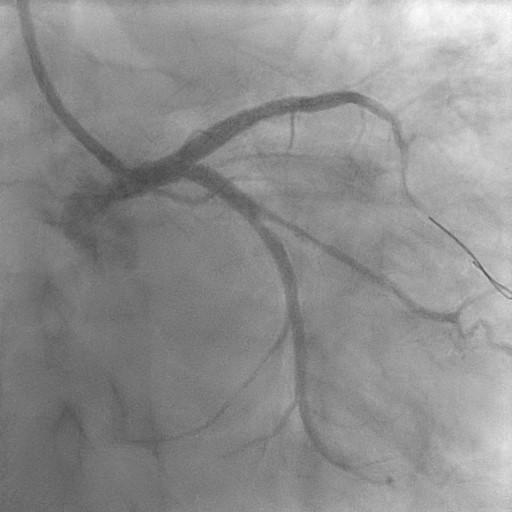
Predilated LAD further with Scoring balloon 2.5/15mm upto14 atm. Stent: Xience Sierra (Abbott) 2.75/33mm at nominal pressure. Cine after stenting: TIMI 3 Flow with possible under-expansion at proximal and mid segment of stent. Post dilated with non-compliant balloon (NC) 3.0/20mm up-to 24 atm. Good final results but patient is complaining of mild chest pain. She is hemodynamically stable with no ECG changes. Visualized further with OCT- good stent apposition, expansion with no distal stent edge dissection. Crossed CTO OM using Run-Through Floppy with balloon support using similar scoring balloon. Drug Coated Balloon: 2.25/35mm after vessel preparation with semi compliant balloon (SC) 1.5/10mm and Scoring balloon 2.0/15mm. Her chest pain got worst with sweating- not improving despite IV Fentanyl 50mcg. Hemodynamically stable. Reviewed back last frame visible before blood swirling in the LMS –vulnerable plaque? It’s a TCFA (thin cap fibroatheroma)! IVUS run shows a dissection in the LMS involving the media extending to ostial LMS, Predilated LMS with NC 3.5/15mm up-to 16atm. Stent: Biofreedom Ultra 3.5/24mm (Biosensors) overlapping LAD stent- chest pain free right after. POT: 4.0/8mm up-to 18 atm. Kissing balloon inflation: 3.5 and 2.5 NC at nominal and Re-POT with 4.0/8mm upto 18atm. IVUS Post: good stent apposition/expansion, MSA-11.81 at LMS. Patient well post procedure and was discharged after 2 days.
Case Summary
Optical Coherence Tomography (OCT) is increasingly used to assess ambiguous lesions and optimize LMS PCI. However, its ability to provide artefact-free high quality images of coronary ostia and large segments such as the LM remains uncertain. Thin-cap fibroatheroma(TCFA) is recognized as a precursor for plaque rupture, which is responsible for the majority of cases of acute coronary syndromes (ACS) and its visualization in LMS is difficult from OCT. This case illustrated catheter induced dissection involving a TCFA in LMS. Using both OCT and IVUS, we optimized the angioplasty of LMS-LAD.