
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-038
An Eventful Rotational Atherectomy Over the Left Main Stem and Left Anterior Descending Artery in an Elderly Male
By Gurpreet Pal Singh Jugindar Singh, Tze Ming Chan, Yew Fung Kwan, Hazleena Mohamed Hasnan, Sabapathy Diagarajan, Mohd Ruslan Mustapa, Kengeswari Raja, Chen Tai Meng, Ramachandran Sathappan, Nor Hanim Mohd Amin
Presenter
Gurpreet Pal Singh Jugindar Singh
Authors
Gurpreet Pal Singh Jugindar Singh1, Tze Ming Chan2, Yew Fung Kwan1, Hazleena Mohamed Hasnan1, Sabapathy Diagarajan3, Mohd Ruslan Mustapa4, Kengeswari Raja1, Chen Tai Meng1, Ramachandran Sathappan5, Nor Hanim Mohd Amin1
Affiliation
Hospital Raja Permaisuri Bainun, Malaysia1, Columbja Asia petaling Jaya, Malaysia2, Hospital Pulau Pinang, Malaysia3, Sultan Idris Shah Serdang Hospital, Malaysia4, Hrpb Ipoh, Malaysia5,
View Study Report
TCTAP C-038
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
An Eventful Rotational Atherectomy Over the Left Main Stem and Left Anterior Descending Artery in an Elderly Male
Gurpreet Pal Singh Jugindar Singh1, Tze Ming Chan2, Yew Fung Kwan1, Hazleena Mohamed Hasnan1, Sabapathy Diagarajan3, Mohd Ruslan Mustapa4, Kengeswari Raja1, Chen Tai Meng1, Ramachandran Sathappan5, Nor Hanim Mohd Amin1
Hospital Raja Permaisuri Bainun, Malaysia1, Columbja Asia petaling Jaya, Malaysia2, Hospital Pulau Pinang, Malaysia3, Sultan Idris Shah Serdang Hospital, Malaysia4, Hrpb Ipoh, Malaysia5,
Clinical Information
Patient initials or Identifier Number
SHS
Relevant Clinical History and Physical Exam
Mr SHS was admitted in August 2022 for acute decompensated heart failure secondary to NSTEMI, complicated with ventricular tachycardia (VT). CPR was performed for6 minutes on the day of admission and was subsequently transferred to the Cardiac Care Unit. His hospital stay was complicated with Covid-19 infection(category 2b) which he recovered well from. During admission, he developed recurrent episodes of angina. Physical examination was otherwise unremarkable. His ejection fraction was 45%.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
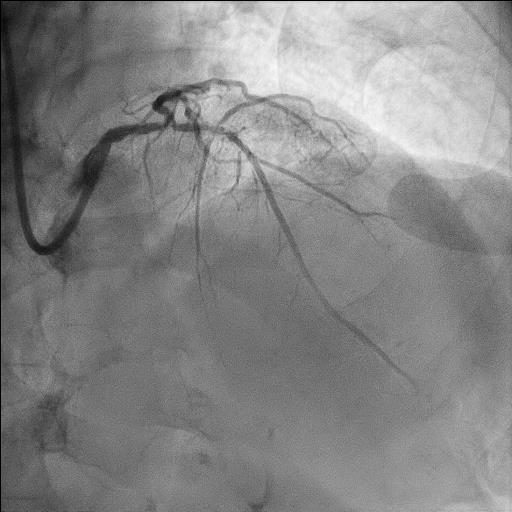
Cardiac catheterization was performed, which revealed significant calcification of left and right coronary arteries. There was a left main stem bifurcation lesion (Medina 0,1,1) with subtotal occlusion over ostial the LAD , receiving collaterals from RCA and 90% stenosis over ostial LCx. RCA was dominant, heavily calcified with no significant stenosis. He was counselled for CABG (Syntex score26) but refused. As he was symptomatic, he was planned for PCI to the left coronary system.
Interventional Management
Procedural Step
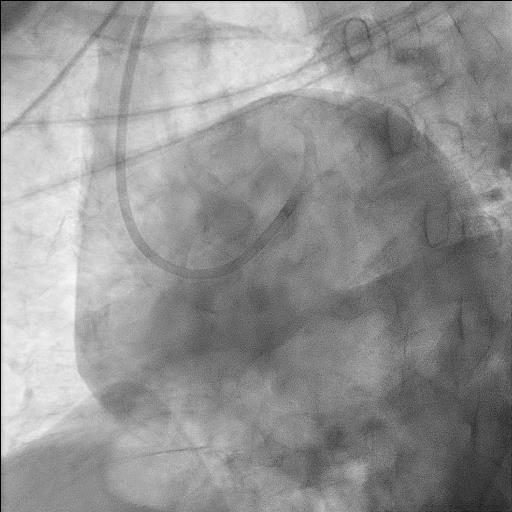
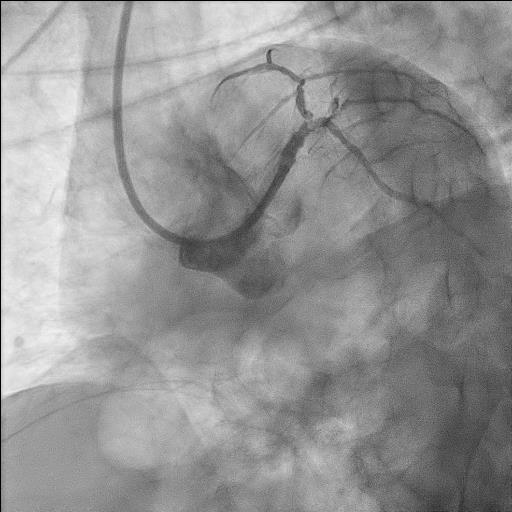
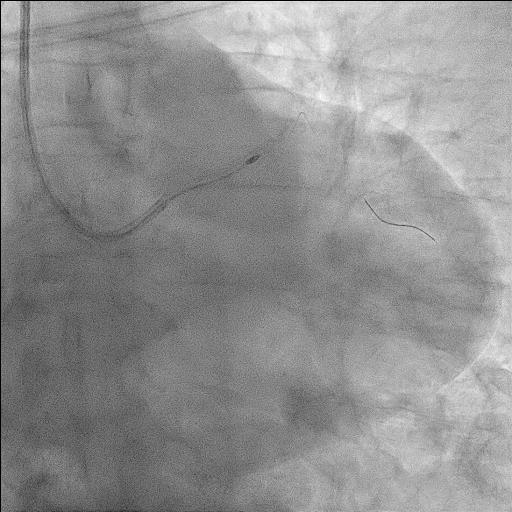
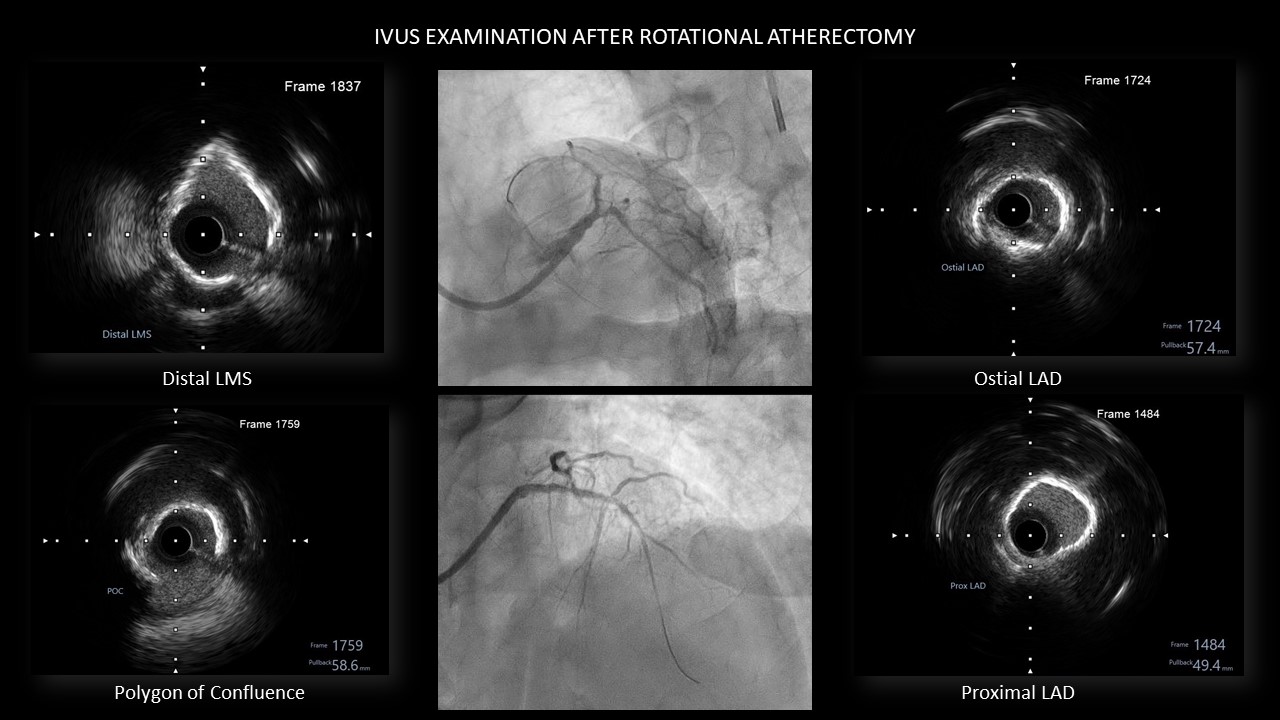
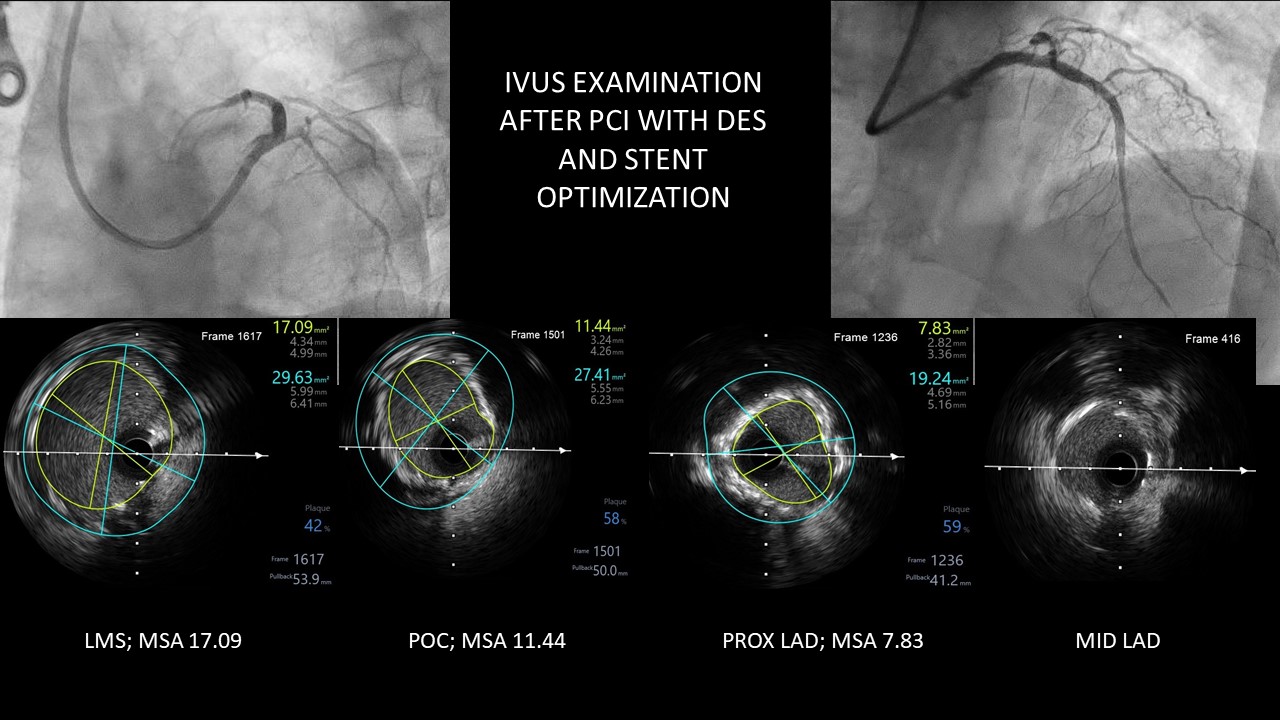
The left main was engaged with a 7F EBU 3.5guiding catheter via transradial approach. Sion Blue wired into LAD and LCx. IVUS catheter couldn’t cross the LAD and LCx lesions, hence we decided for up front rotational atherectomy. Sion blue was exchanged to Rotawire with the assistance of Finecross microcatheter. A 1.5mm burr was used at 180000 rpm. After the first run of rotablation, patient developed chest pain and severe hypotension (BP ranging 50/30). 4 inotropes/vasopressors were commenced. The shock was refractory hence an intraarterial balloon pump was inserted. Symptoms and blood pressure improved. Another 2 runs of atherectomy done (patient developed hypotension after each run). IVUS examination then showed calcification of proximal to mid LAD with an IVUS Calcium score of 3. LAD was further predilated with Scoreflex balloon 3.0/20mm at 8–22ATM. LCx was predilated with Scoreflex balloon 2.0/15mm at 12–14ATM. DCB Sequent Please NEO2.0/30mm was deployed at 7ATM at ostial to proximal LCx. Proximal to mid LAD was stented with Promus ELITE 2.5/32mm at 11ATM, which was then post dilated with stent balloon at 11ATM. Ostial LM to proximal LAD (overlap) was stented with Promus ELITE 4.0/28mm at 11ATM. LMS POT was then done with NC Balloon 4.0/15mm at 24ATM. LCx was rewired and kissing balloon technique with NC balloon 4.0/15mm at 14ATM (LAD) and NC balloon 2.0/10mm at 12ATM (LCx) was done, followed by a final POT with NC balloon 4.0/15mm at 14ATM. Final IVUS showed good MSA.
Case Summary
This patient developed hemodynamic instability with each rotational atherectomy run, hence we decided not to perform rotablation to the circumflex artery. His hemodynamic condition improved with the use of intra aortic balloon pump. IABP use can reduce procedural event rate and potentially reduce long term mortality in appropriately selected patients who are at high risk of adverse events. He was followed up a month following the procedure and remained asymptomatic. For complex, calcified coronary lesions involving the left main stem, coronary artery bypass graft surgery is an alternative option.