
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-126
Saphenous Vein Graft Perforation in an Acute Coronary Syndrome Patient With Large Thrombi
By Yi Pan Li
Presenter
Yi Pan Li
Authors
Yi Pan Li1
Affiliation
National Cheng Kung University Hospital, Taiwan1,
View Study Report
TCTAP C-126
CORONARY - Complications (Coronary)
Saphenous Vein Graft Perforation in an Acute Coronary Syndrome Patient With Large Thrombi
Yi Pan Li1
National Cheng Kung University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Mr. Lan
Relevant Clinical History and Physical Exam
This 86-year-old man with the history of diabetes and coronary artery disease undergoing coronary artery bypass surgery 19 years ago complaint of acute onset of chest pain in the morning. The pain couldn't be relieved by sublingual nitroglycerin. The initial vital signs were T/P/R: 36.5 degrees /113 bpm/18 bpm and the blood pressure was 147/90 mmHg. The physical examination showed regular heart beat without audible murmurs or basal crackles.
Relevant Test Results Prior to Catheterization
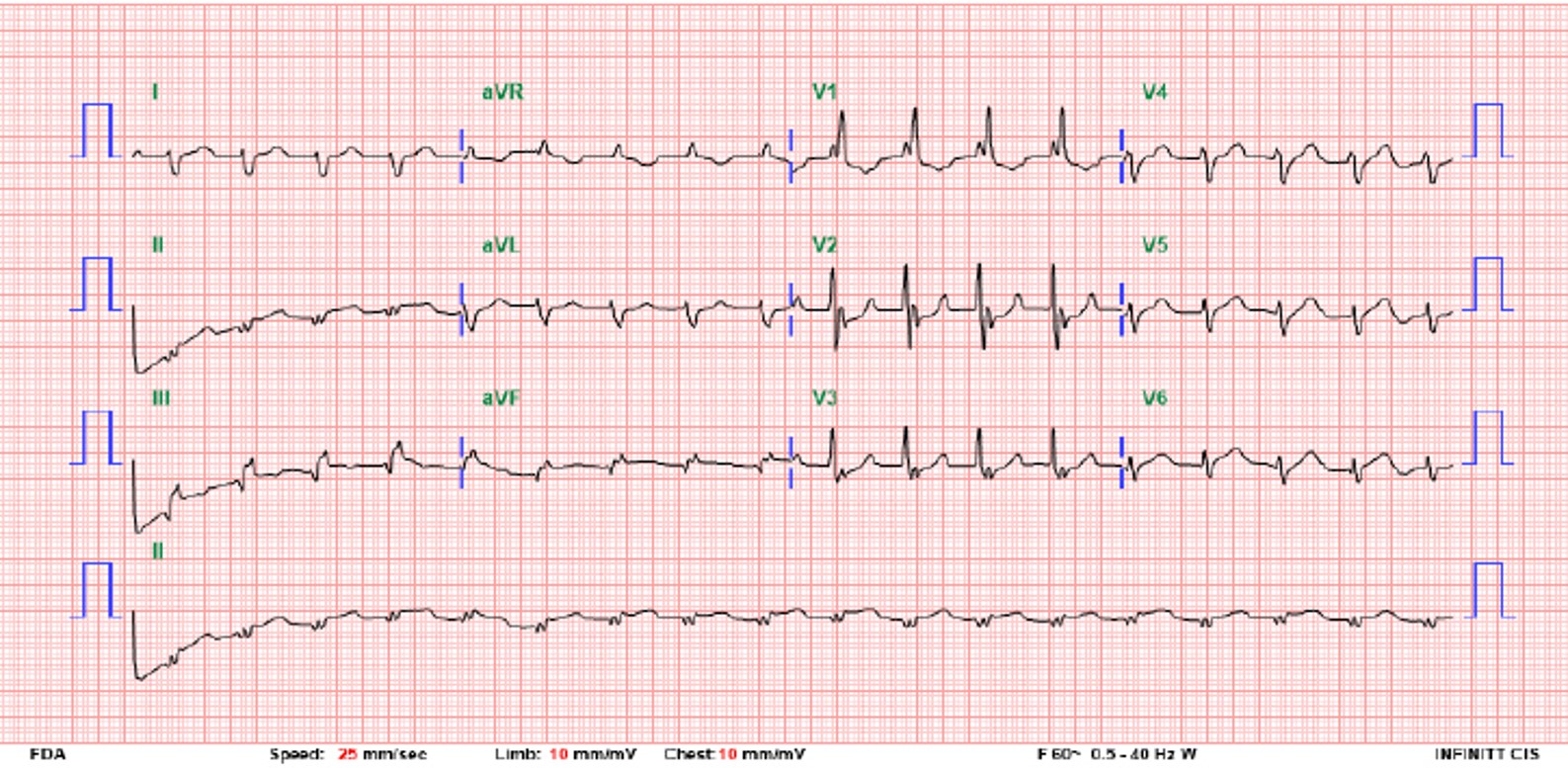
The ECG showed sinus rhythm with right bundle branch block and suspected ST elevation in inferior leads. The echocardiography showed impaired LV systolic function with inferior and inferolateral hypokinesis. The CK-MB was 5.7 ng/mL and the hs-TnT was 180.3 ng/mL. After loading aspirin, clopidogrel and heparin, he underwent primary percutaneous coronary intervention.
Relevant Catheterization Findings
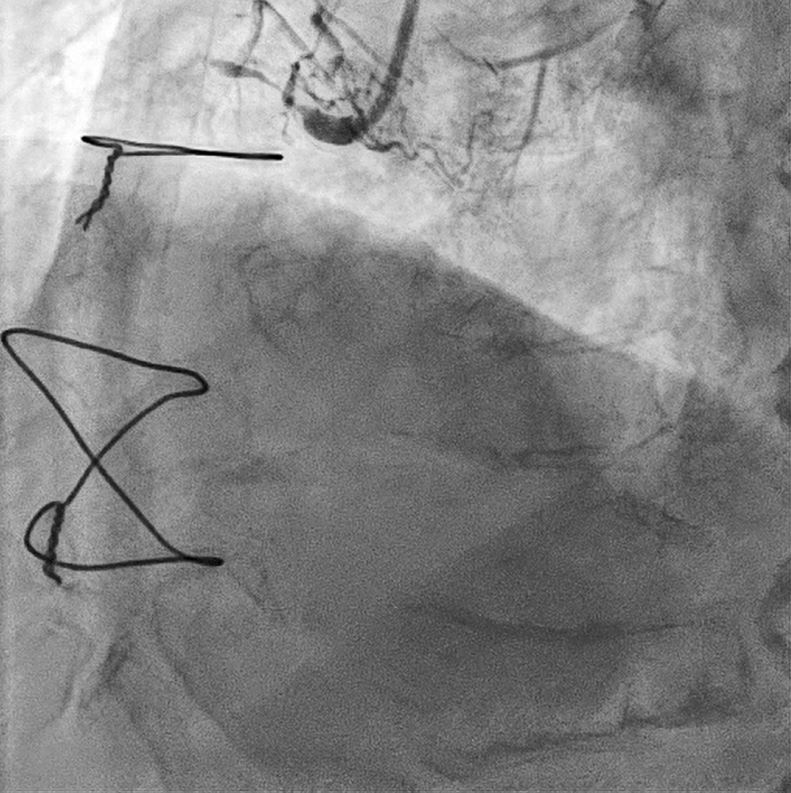
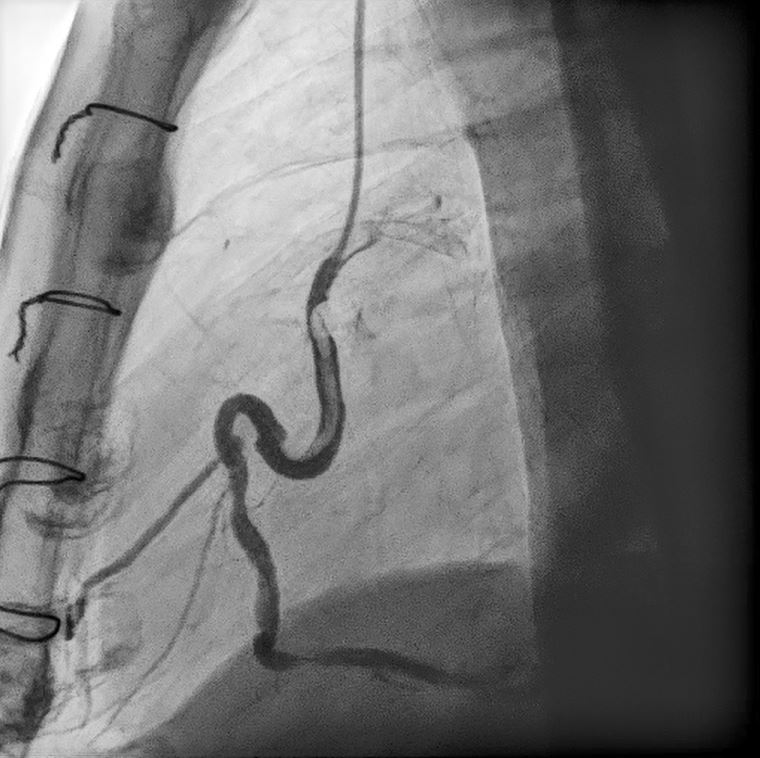
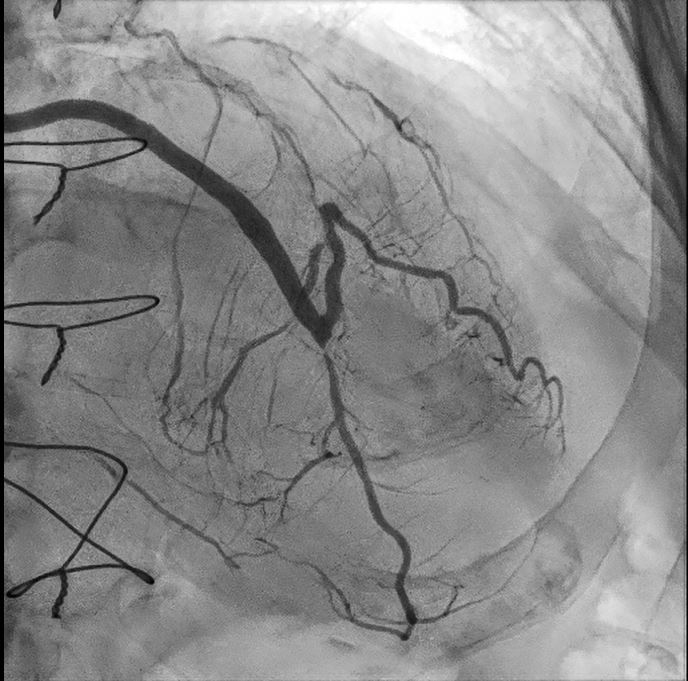
Left Main: Total occlusion at orificeLAD: Total occlusion at orifice, post stenting at proximal LADLCX: Total occlusion at orificeRCA: Total occlusion at orificeSVG1 to dLAD: A 70% stenosis at the anastomosis site; The flow go back to middle LAD and Diagonal 1 branchSVG2 to RCA: tortuosity with a 70% stenosis and acute thrombosis at proximal partCollateral: LAD septal branches to RCA
Interventional Management
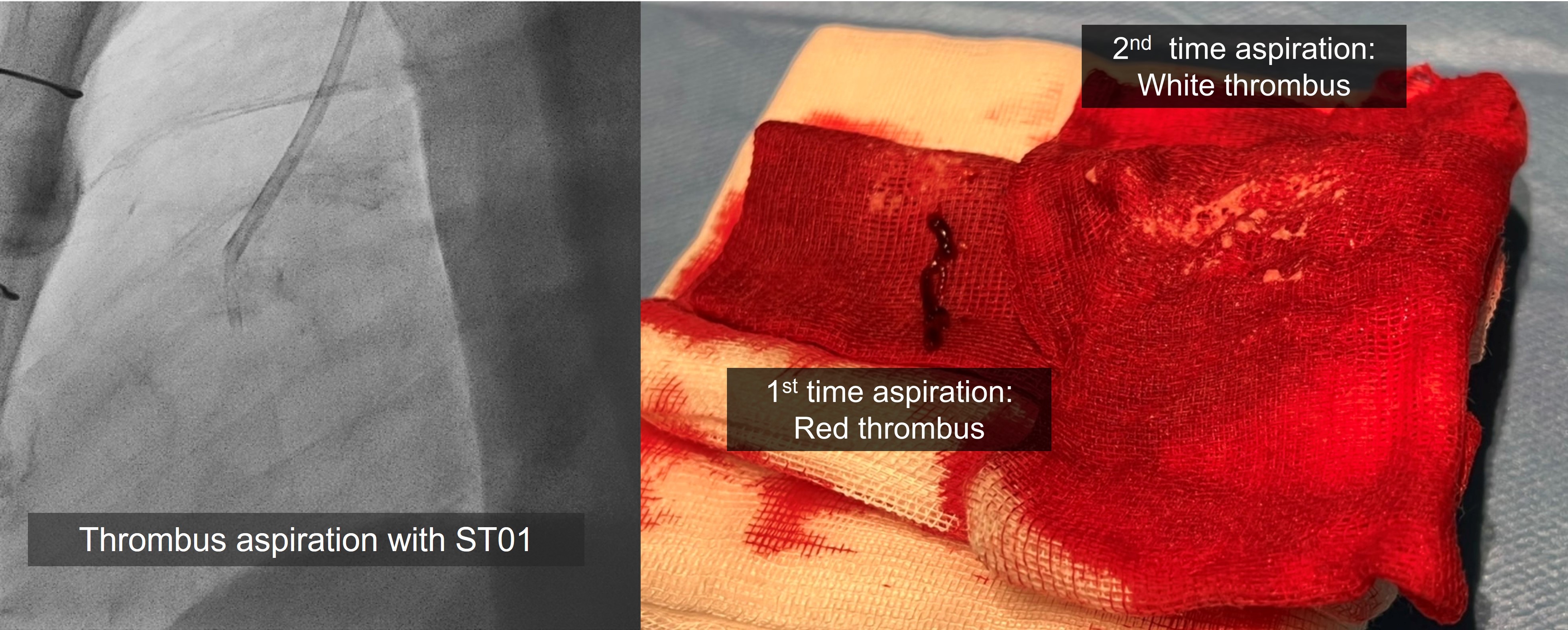
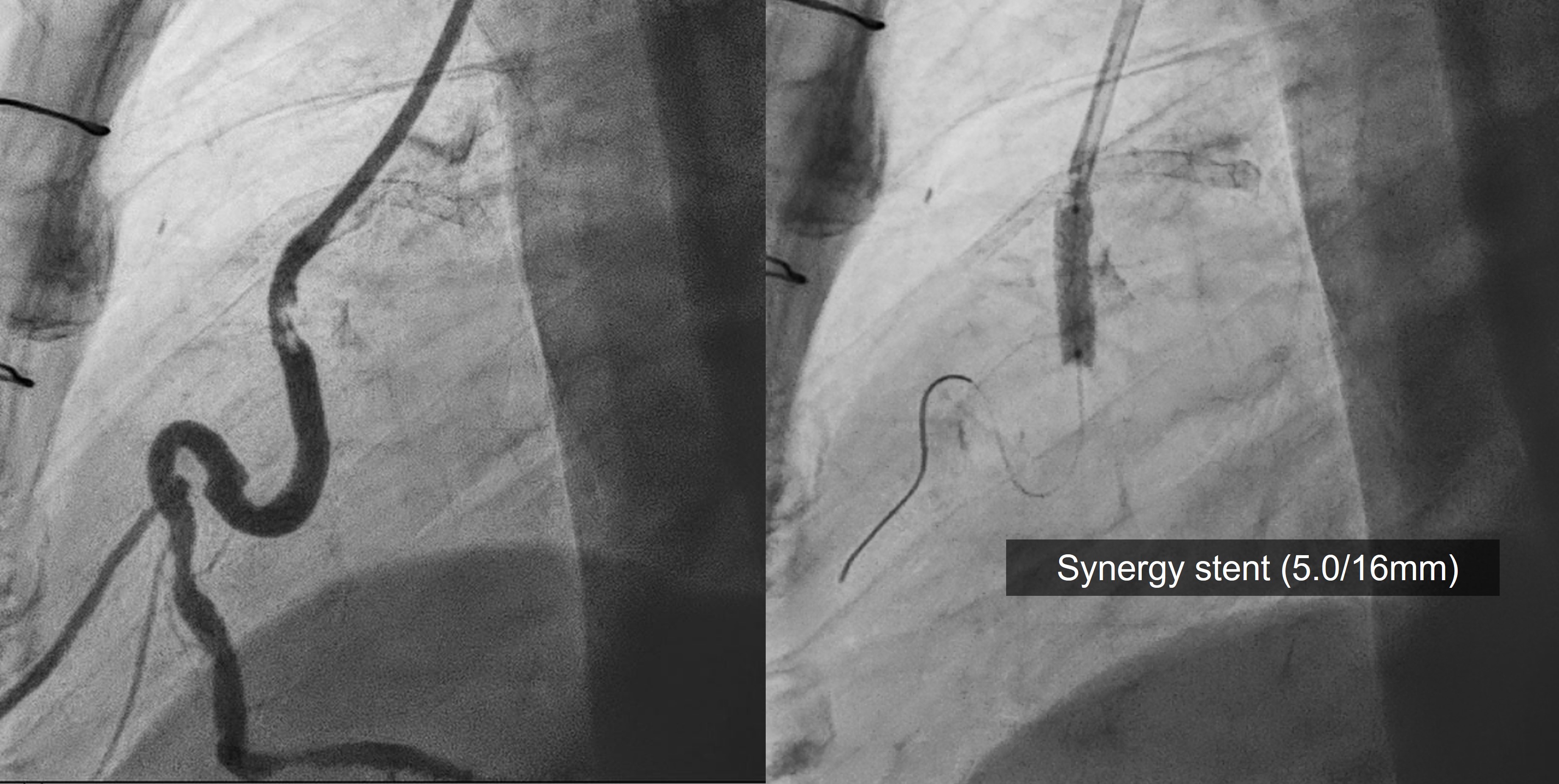
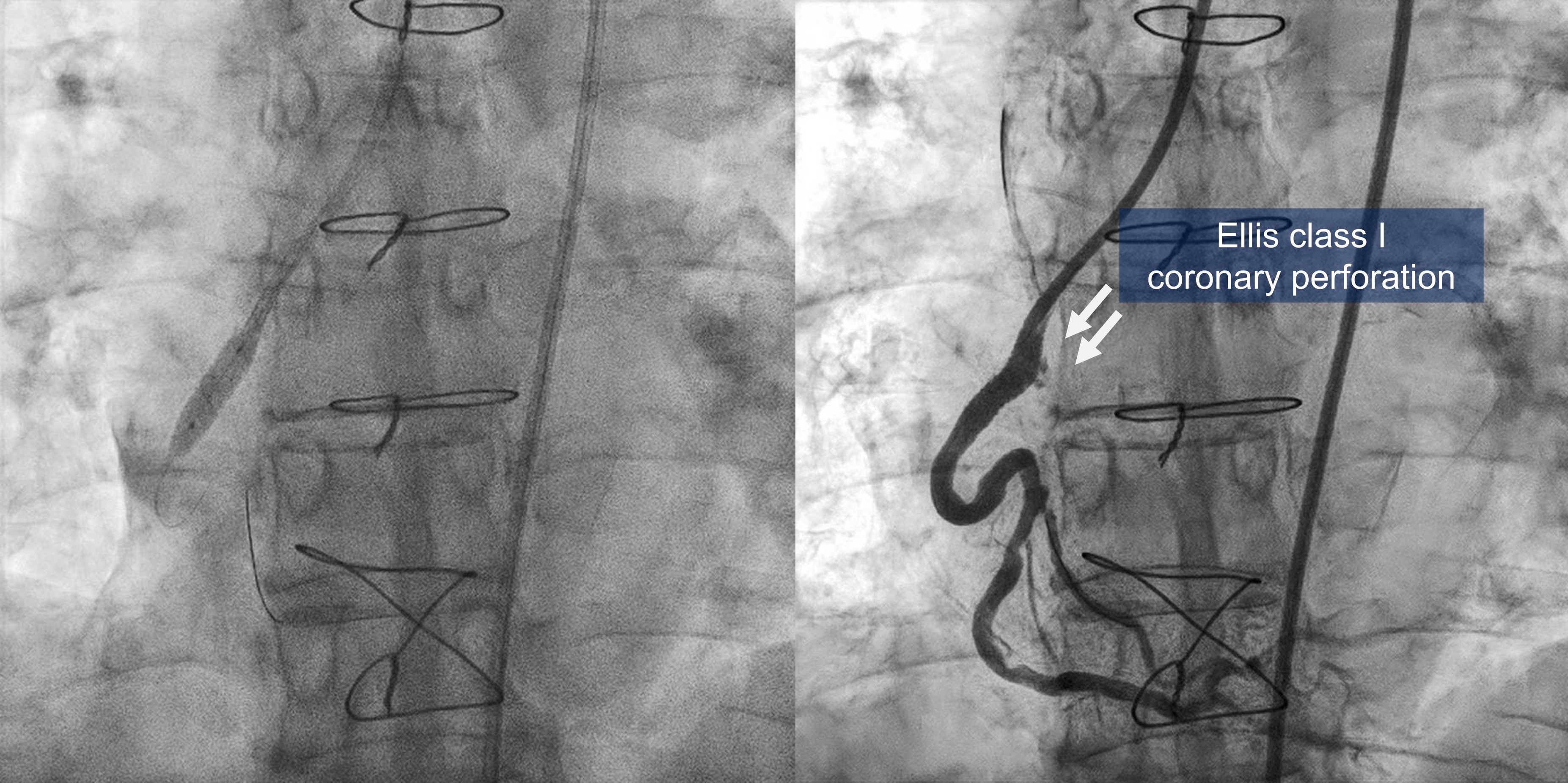
Procedural Step
We used a multipose (7Fr) guide catheter to engage SVG2. The ST01 catheter was advanced to the proximal SVG2 for thrombus suction twice. A red and atherosclerotic plaque (or white thrombus) were aspirated. A Filter EZ wire failed to be advanced and deployed due to tortuosity. A Synergy stent (5.0/16mm) was deployed at proximal SVG. We performed post-dilation with a NC Emerge balloon with 20 atm; however, there was stent deformity during balloon inflation. We found that we used 5.5 mm NC balloon for post-dilation by mistake rather than 5.0mm NC balloon. The angiogram showed an Ellis class I coronary perfoaration. We performed prolonged balloon inflation with low pressure for 3 minutes and administered protamine 2 mg. There was no further extravasation thereafter.
Case Summary
The 86 y/o man with large thrombi at proximal SVG. We did thrombus aspiration with ST01 catheter. We failed to deploy an embolization protection device. A DES was deployed at proximal SVG. During post-dilation, the oversize balloon caused Ellis class I coronary perforation in SVG. We did prolonged balloon inflation and reversed anticoagulation. There was no further extravasation or cardiac tamponade. Prior CABG may protect against progression to tamponade due to the presence of pericardial adhesion. Besides, the proximal SVG segments possibly, locates in extra-pericardial space, preventing pericardial effusion. We have to notice the balloon size during inflation to prevent vessel perforation.