
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-097
When It Rains, It Pours: A Complication Case After Acute Coronary Syndrome
By Yan-Siou Chen, Ying-Hsien Chen, Chih-Fan Yeh, Hsien-Li Kao
Presenter
Yan-Siou Chen
Authors
Yan-Siou Chen1, Ying-Hsien Chen1, Chih-Fan Yeh1, Hsien-Li Kao1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-097
CORONARY - Complications (Coronary)
When It Rains, It Pours: A Complication Case After Acute Coronary Syndrome
Yan-Siou Chen1, Ying-Hsien Chen1, Chih-Fan Yeh1, Hsien-Li Kao1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
6741275
Relevant Clinical History and Physical Exam
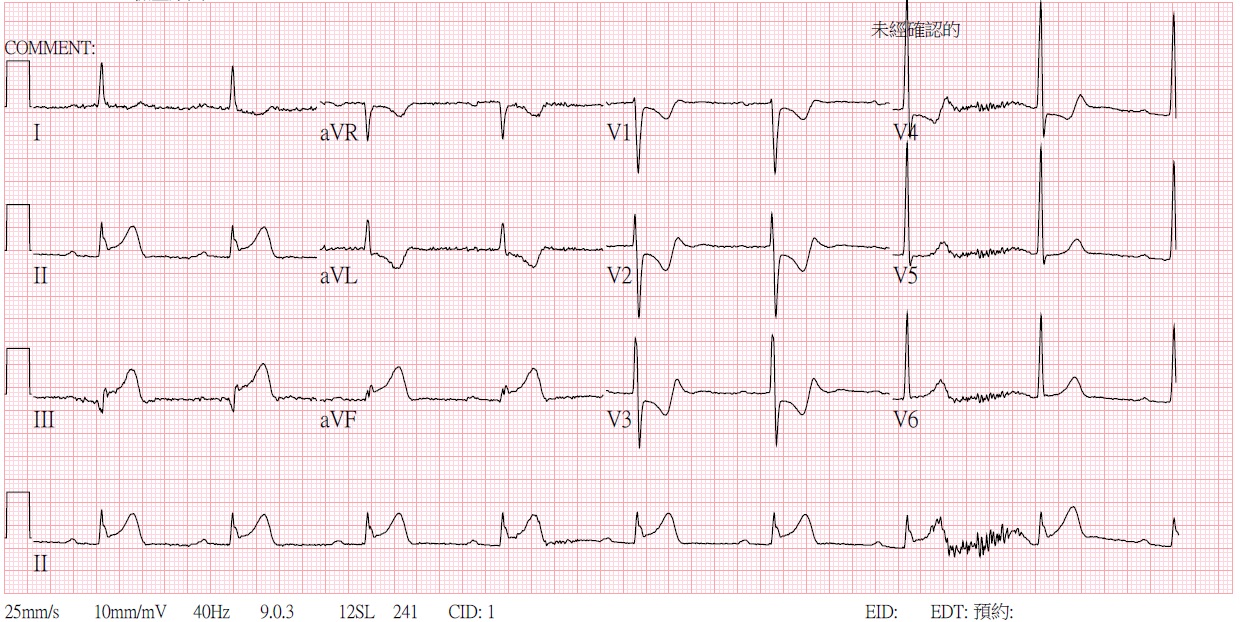
The 70-year-old man with a history of uncontrolled hypertension presented to our hospital due to sudden onset of severe chest pain for 40 minutes with diaphoresis. The vital signs revealed hypotension (96/57 mmHg) and sinus bradycardia. Physical examination showed bilateral clear breathing sound, regular heart beat without significant cardiac murmur and warm limbs without pitting edema. The ECG disclosed sinus rhythm and inferior lead ST-segment elevation with reciprocal ST depression at V1-V5.
Relevant Test Results Prior to Catheterization
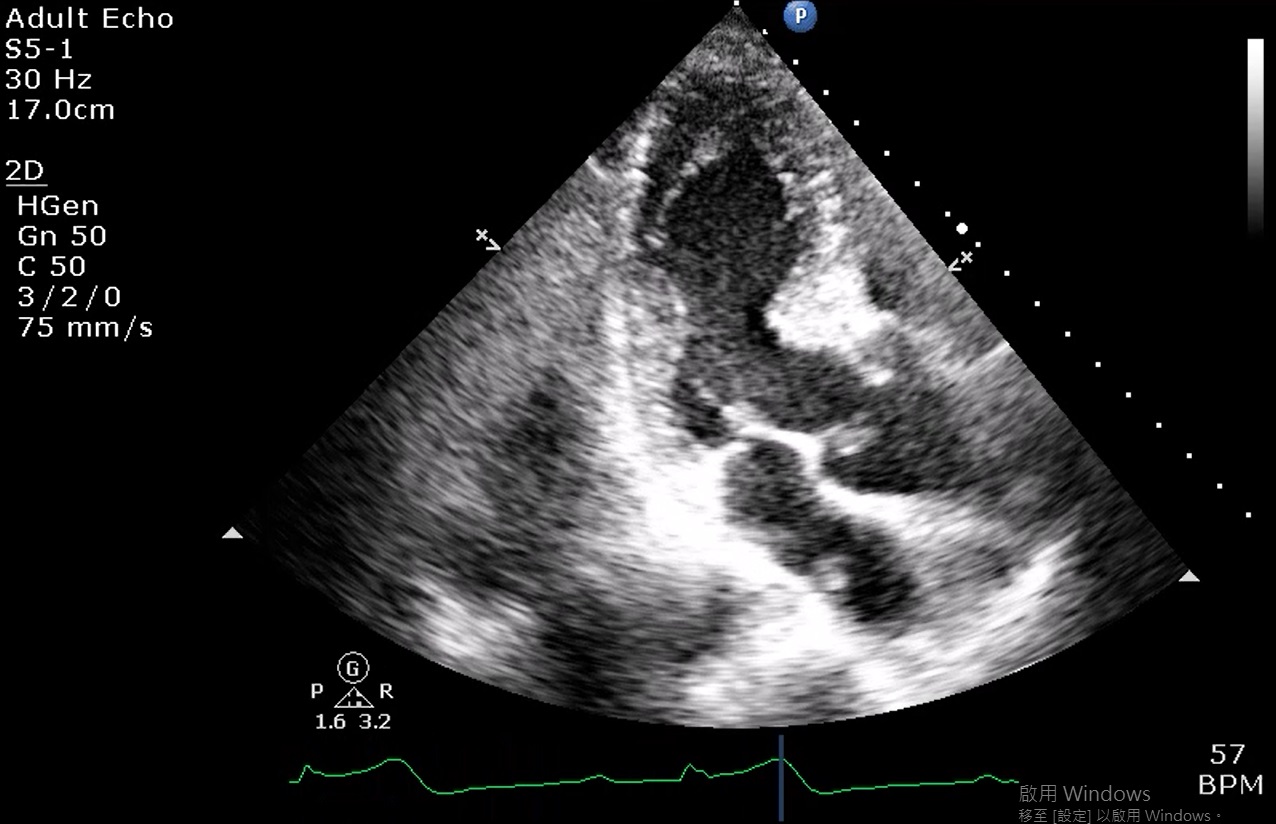
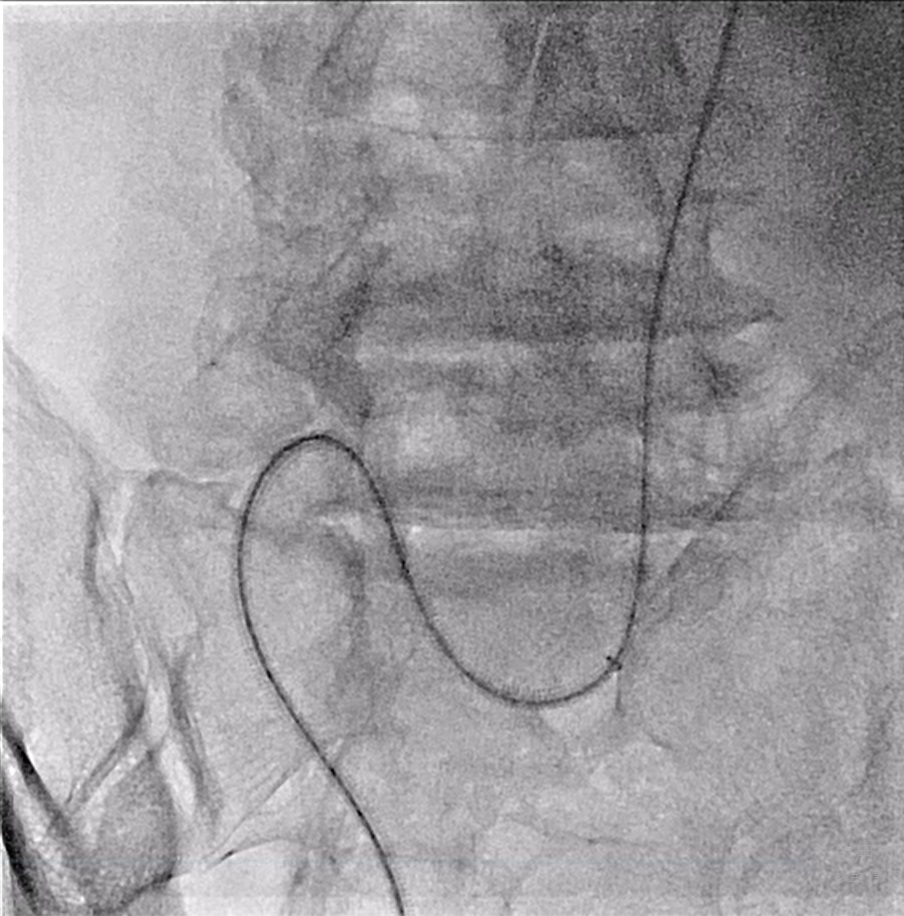
Abnormal regional wall motion at inferior wall was found by ultrasound cardiography. Laboratory tests showed a normal range of hemoglobin (14.7 g/dL), elevating troponin-T (27 ng/L) and impaired renal function (creatinine 1.5 mg/dL). Emergent percutaneous coronary intervention was initiated immediately. From right femoral artery access, due to failure of wiring to aorta, an extremely tortuous at right common iliac artery (CIA) was found, therefore the sheath was replaced to a 45cm 7Fr sheath.

Relevant Catheterization Findings
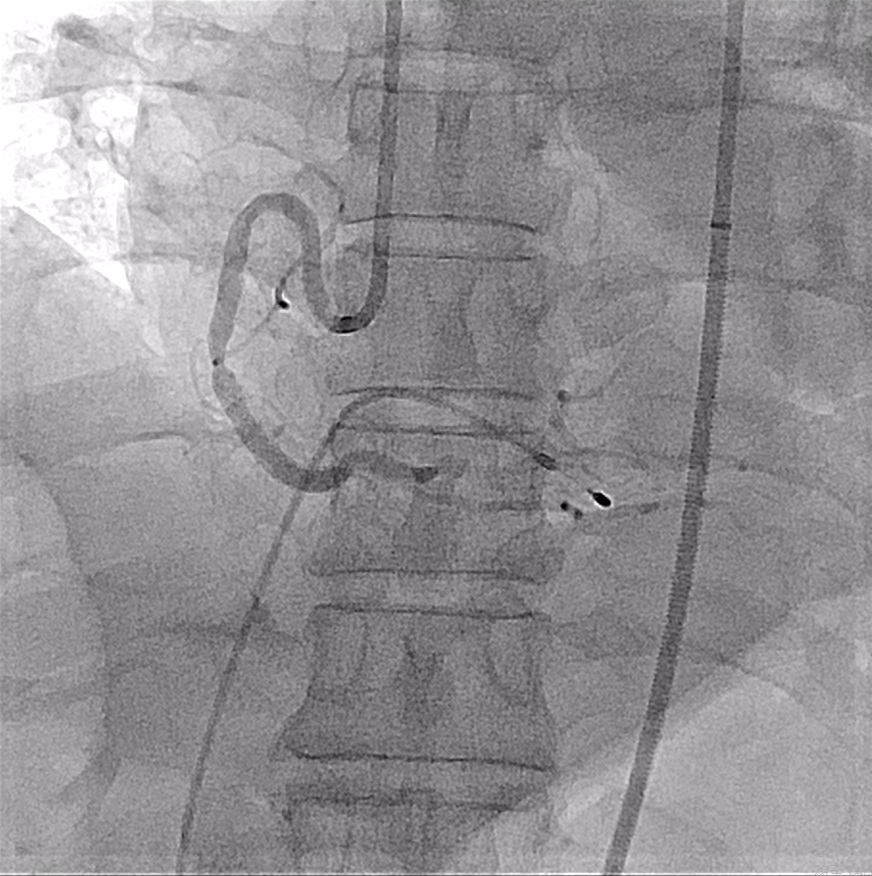
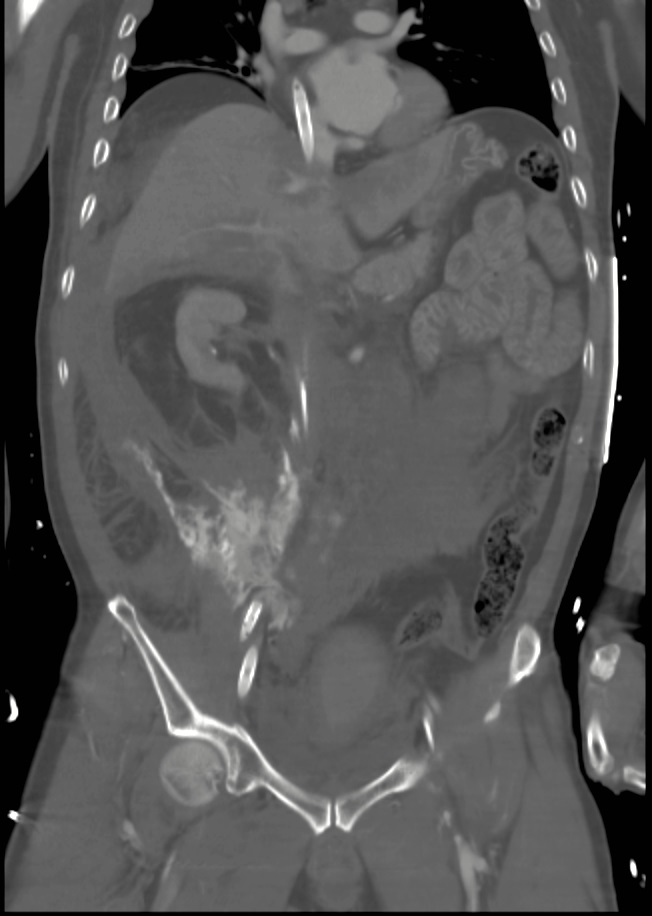
Coronary angiography showed a critical lesion of middle RCA and a drug-eluting stent was deployed smoothly. However, bradycardia with severe shock soon occurred. VA-ECMO was set up for suspected cardiogenic shock, but later the lab test disclosed a significant drop of hemoglobin to 2.7 mg/dL. The blood pressure merely kept at 40/20 mmHg under strong doses of multiple inotropes. An emergent CT scan revealed extravasation at the right CIA, just at the tip of the artery cannula.
Interventional Management
Procedural Step
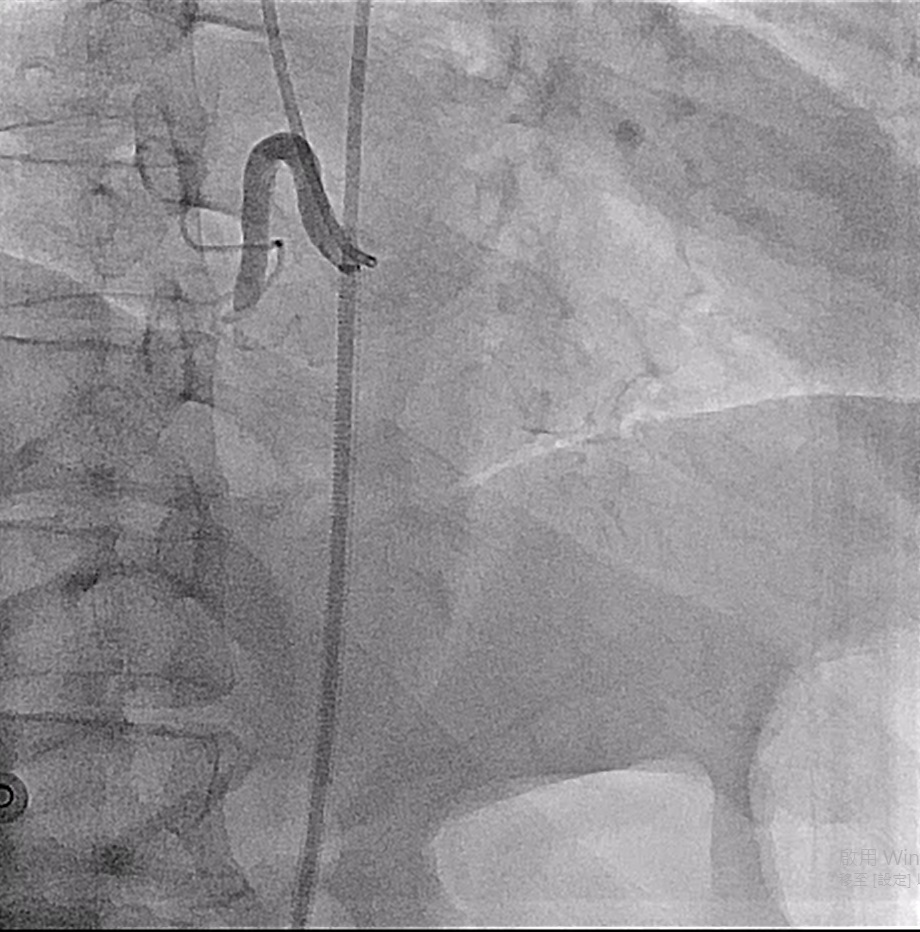
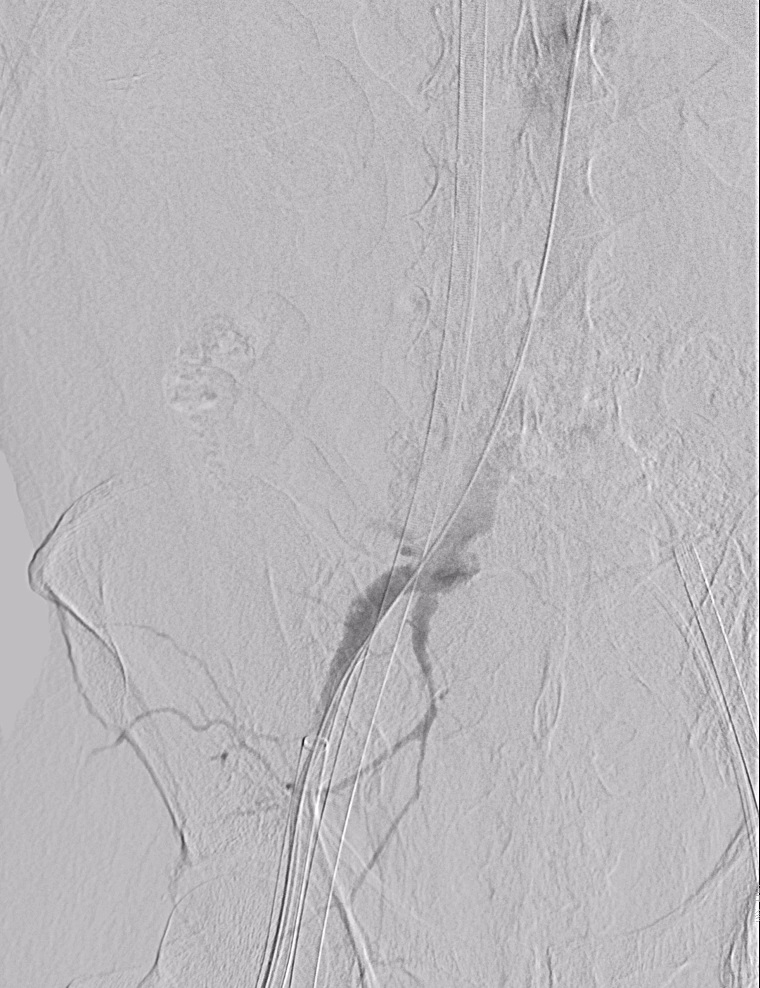
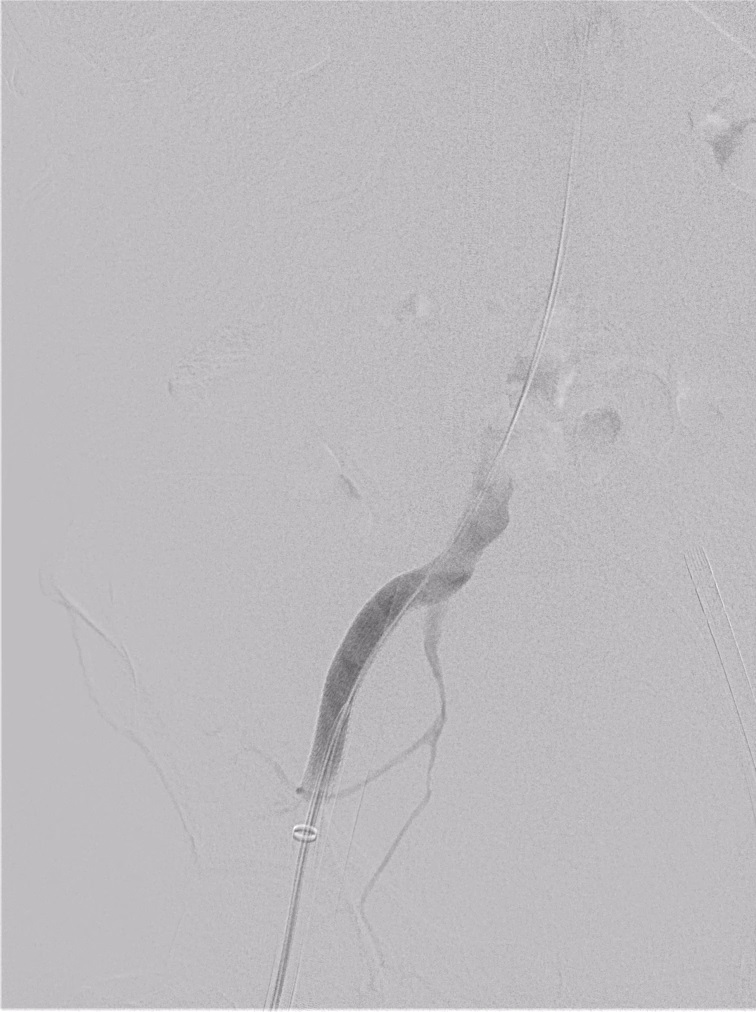
The VA-ECMO was essential to maintain the patient’s vital signs, however, the blood flow from the artery cannula (2.5 L/min) also caused more blood loss and severe extravasation. The patient was sent back to the cath room immediately. The initial angiogram confirmed Step 1: Keep VA-ECMO function: Under ultrasound guidance, we inserted an artery cannula at left common femoral artery (CFA) and connected it to ECMO pump as a new inflow cannula. Step 2: Then we needed secure access to deploy a covered stent. How to exchange the original right CFA cannula to a one-way valve sheath? A 6 Fr sheath was inserted at the right brachial artery. Antegradely wired from right brachial artery to the right CIA, and exited from the right CFA cannula with rendezvous technique, which established a thorough access. Step 3: Exchanged artery cannula to a 18 Fr Dryseal Sheath. After deploying a 13mmx 10cm Viabahn stent at the right CIA, the angiogram showed hemostasis successfully. Step 4: Performed retroperitoneal hematoma evacuation. The blood pressure gradually recovered and all of the inotropic agents were tapered off, thus we decided to remove ECMO.Step 5: Inserted a 7Fr sheath to the left superficial femoral artery (SFA). Removed ECMO artery cannula and deployed 7 mm x 5 mm Viabahn stent to left CFA. Crossover wired to the right CFA. Removed the rigth CFA 18 Fr sheath and deployed another 8 mm x 10 mm Viabahn stent. Removed the left SFA sheath and closed the wound with Angio-Seal closure device.

Case Summary
Cardiogenic shock is often seen in acute coronary syndrome, and a VA-ECMO is a reasonable choice for temporary mechanical support. However, retroperitoneal hemorrhage may also occur in femoral access up to 0.2%, with a higher risk in tortuous iliofemoral artery. When the VA-ECMO meets retroperitoneal hemorrhage, it turns into a life-threatening and complicated condition. We shared a different strategy to establish a safe route for stent deployment during the critical condition, and successfully prevented the lethal hemorrhagic shock. It is also an important lesson to early detect potential complications and differentiate the causes of shock before an invasive mechanical circulatory support.