
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-073
Which Microcatheter to Use for Tip-in Method During Complex Percutaneous Coronary Intervention?
By Tien-Chien Tsai, Wen-Lieng Lee
Presenter
Tien-Chien Tsai
Authors
Tien-Chien Tsai1, Wen-Lieng Lee1
Affiliation
Taichung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-073
CORONARY - Chronic Total Occlusion
Which Microcatheter to Use for Tip-in Method During Complex Percutaneous Coronary Intervention?
Tien-Chien Tsai1, Wen-Lieng Lee1
Taichung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Mr. Liu
Relevant Clinical History and Physical Exam
This is a 42-year-old male with history of paroxysmal atrial fibrillation, CAD and hyperthyroidism. He suffered from intermittent chest tightness and short of breath on exertion. He underwent ablation for paroxysmal fibrillation and CAG was performed after ablation. Physical examination showed regular heart beat and S4 gallop.
Relevant Test Results Prior to Catheterization
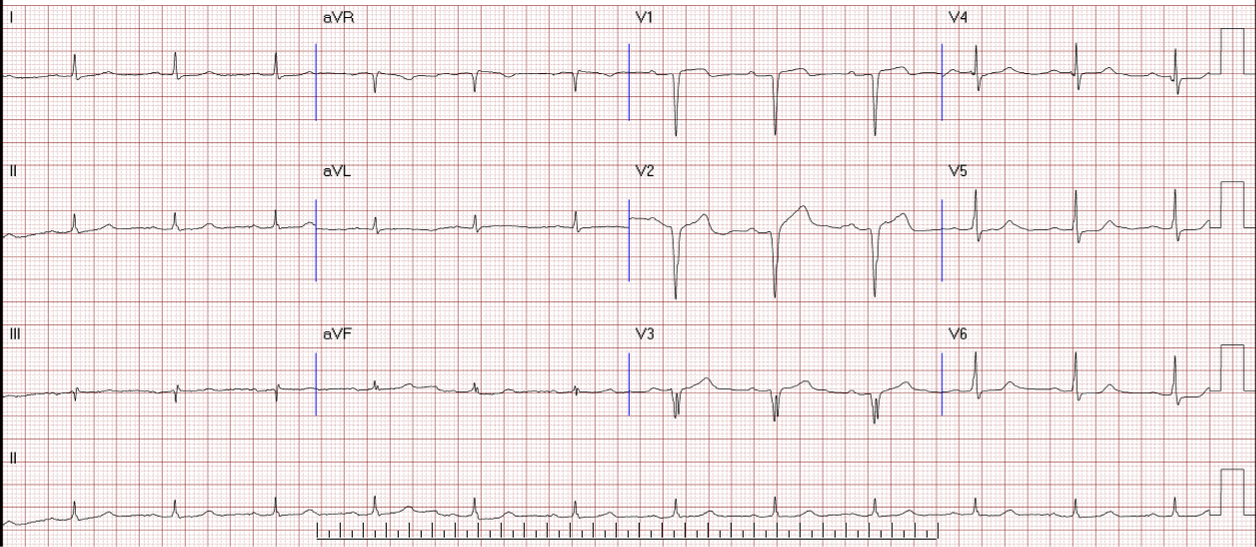
Chest x ray revealed no cardiomegaly and mild infiltration. ECG disclosed sinus rhythm and Q wave over pericardial lead.

Relevant Catheterization Findings
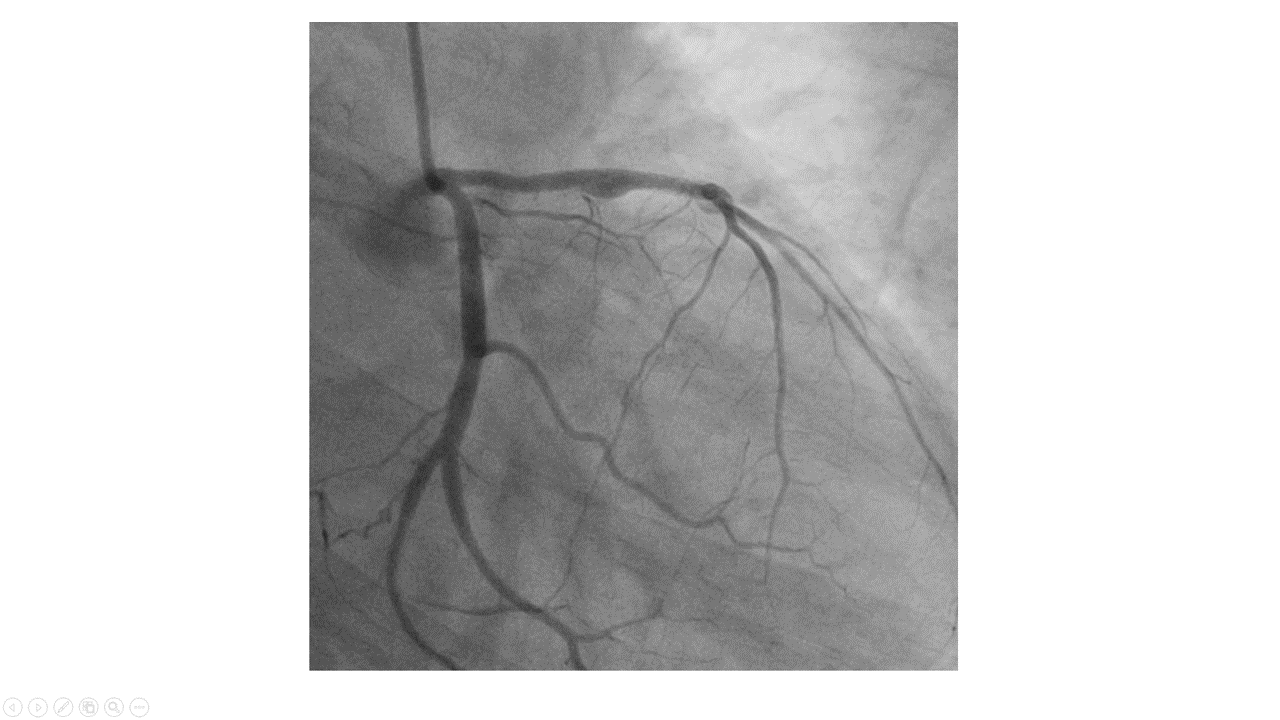
CAG showed CAD-II, LAD-P to -M: instent restenosis over distal stent part, about 50-60% ISR, with collaterals from LAD-D to RCA PDA, RCA-proximal: CTO with stump with auto-collaterals from SAN branch to RV branch, collaterals from LAD-D to RCA-PDA.

Interventional Management
Procedural Step
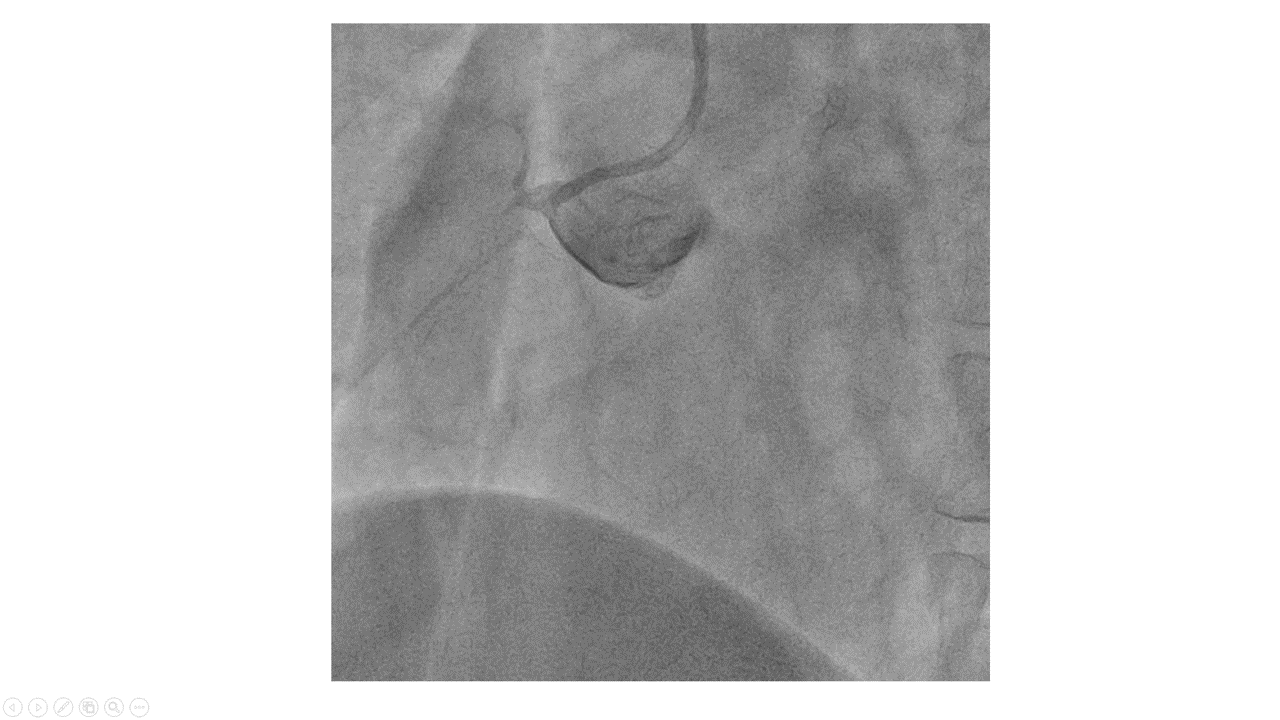
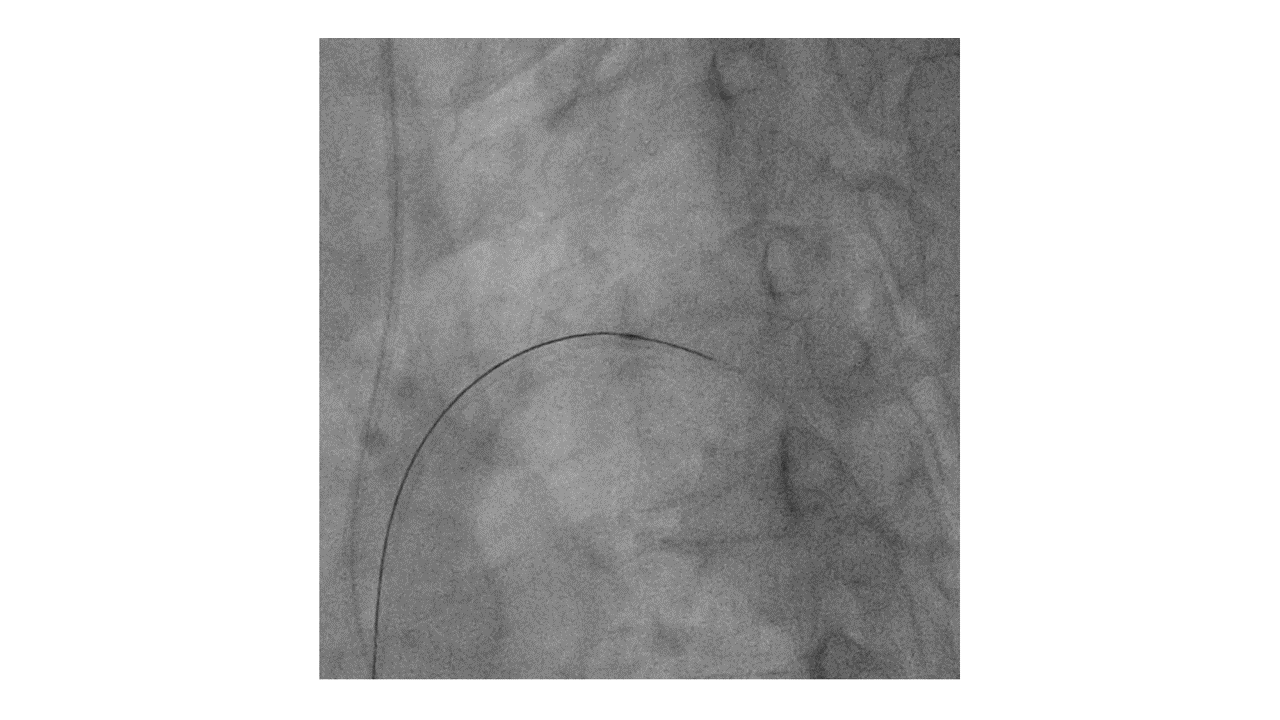
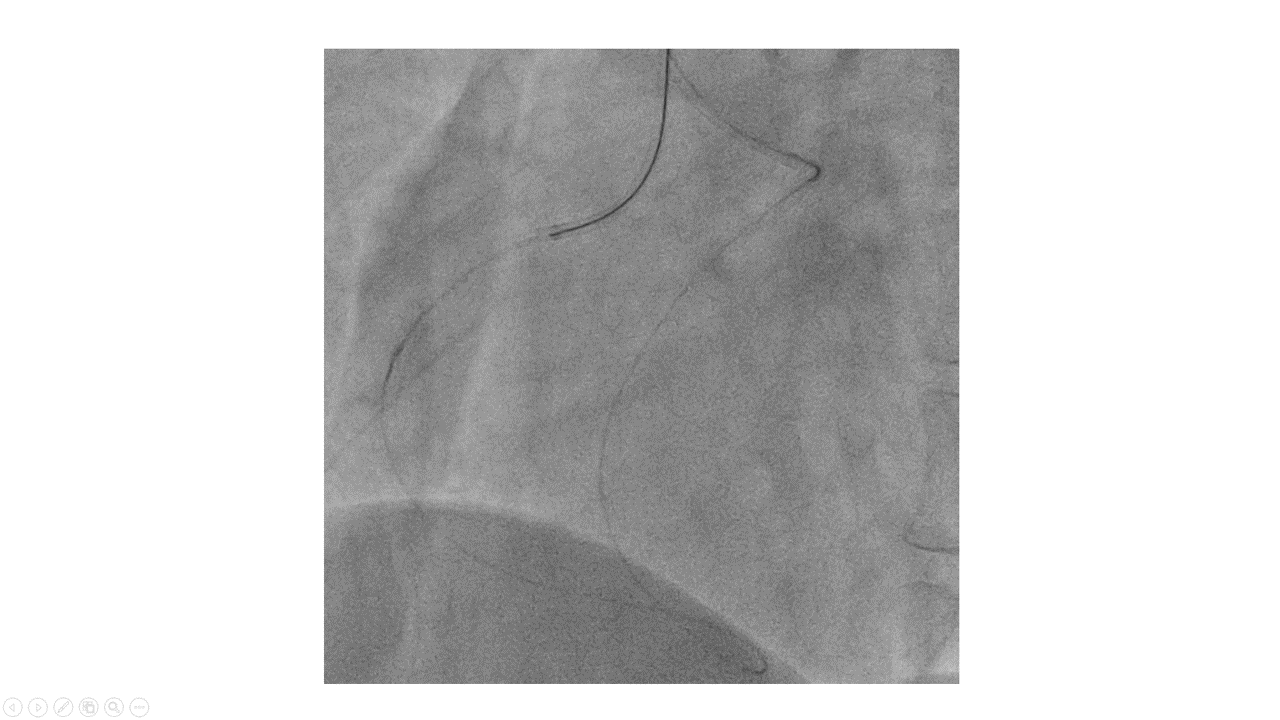
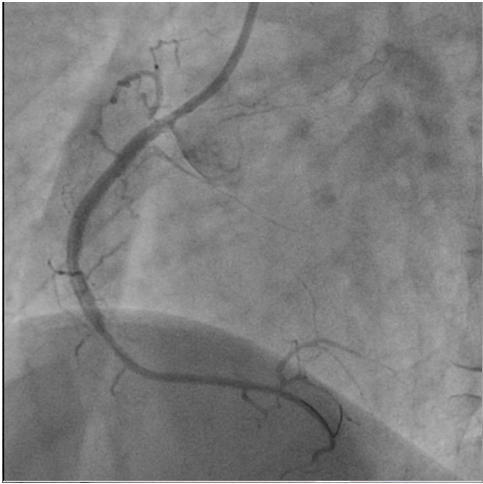
Antegrade approach was approached sequentially with AR 2x6F and SAL 1.5x6F guide via right radial access. However, the proximal CAP was very hard and failed to be correctly crossed with either Fielder XT-A (Asahi, Japan), Conquest Pro (Asahi, Japan) or Pro 820 (Asahi, Japan). Then retroapproach followed. Retrograde approach was done with an XB 3x6F guide via right femoral access. The septal collateral could be easily wired with a broken-tip Sion, followed by advancement of the Caravelle (Asahi, Japan) to distal CTO cap. Retro wiring could be made with an UB 3 (Asahi, Japan), but retro Caravelle failed to followed. After UB 3 went into the antegrade SCR 3.5x6F guide, Tip-in tech was made into an anteCaravelle, but it failed to go through the CTO cap. Tipping into a Tornus (Asahi, Japan) failed due to too tiny lumen of the Tornus. Tipping into a Turnpike gold (Teleflex, US) succeeded, and the Turnpike Gold could be advanced into the CTO body. Antegrade wiring was successfully made with a Conquest Pro. The whole lesion was sequentially dilated with a 1.5x20 mm and a 2x30 mm BC, inflated up to 10 bars. Finally, the whole lesion was scaffolded with a 2.5x48 mm drug-eluting stent, inflated up to 18 bars and post dilated with a 3x20 mm NC BC, inflated up to 20 bars. Final coronary angiography revealed no residual stenosis, good final flow and no collateral damage via contralateral injection.
Case Summary
Calcified spot could be the door to a safety vault and has to be overcome before procedure success. Tip in to a Tornus catheter could be very difficult for a hard wire with sharp and tiny tip curve. Tip in to a Turnpike Gold catheter could be a much better alternative in such circumstance and Turnpike Gold catheter is itself a better choice for calcium.