
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-034
Calcium Nodule in In-Stent Restenosis: Combination of Rotablation and Shockwave Intravascular Lithotripsy
By Yik Ching Hung
Presenter
Yik Ching Hung
Authors
Yik Ching Hung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1,
View Study Report
TCTAP C-034
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Calcium Nodule in In-Stent Restenosis: Combination of Rotablation and Shockwave Intravascular Lithotripsy
Yik Ching Hung1
Tuen Mun Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
LMT
Relevant Clinical History and Physical Exam
A 74-year-old lady, with history of hypertension and hyperlipidrmia, had IVUS guided PCI done in November 2021 for NSTEMI, during which stenting was performed at ostial to mid RCA. She came to us again August 2022 for few days history of anginal chest pain. Her blood pressure and pulse were all along stable after admission.
Relevant Test Results Prior to Catheterization
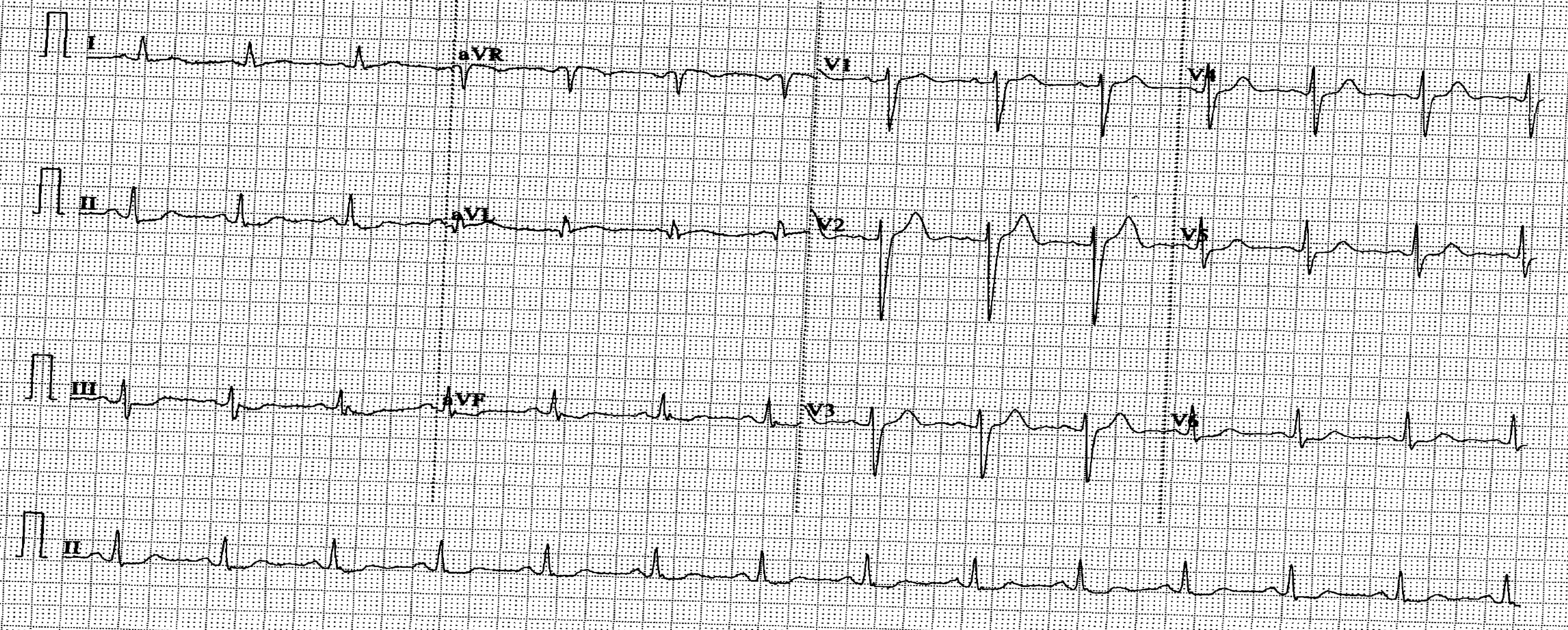
ECG showed no acute ischemic changes. Serial high sensitive-troponin I raised from 84 to 135 ng/L, taken 5 hours apart. Echocardiogram showed normal left ventricular systolic function at 64% with no regional wall motion artefact.
Relevant Catheterization Findings
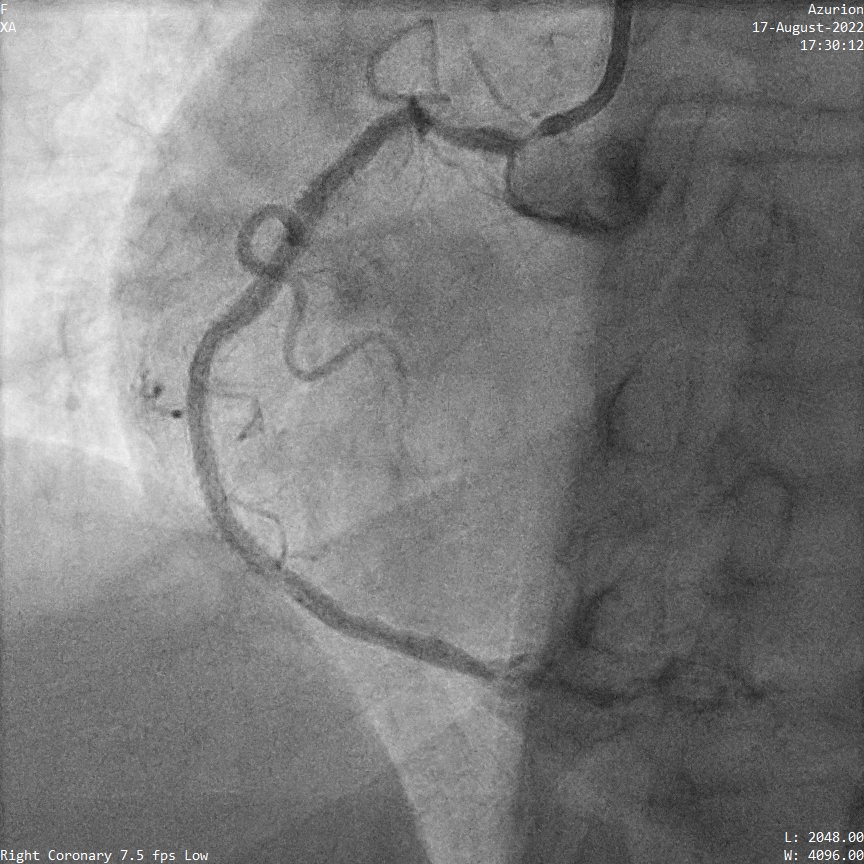
Coronary angiogram showed 40% stenosis at proximal LAD, minor disease at LCX and 80-90% in-steent restenosis from proximal to mid RCA.
IVUS to RCA showed a calcium nodule at outer curve of proximal RCA causing in-stent restenosis.
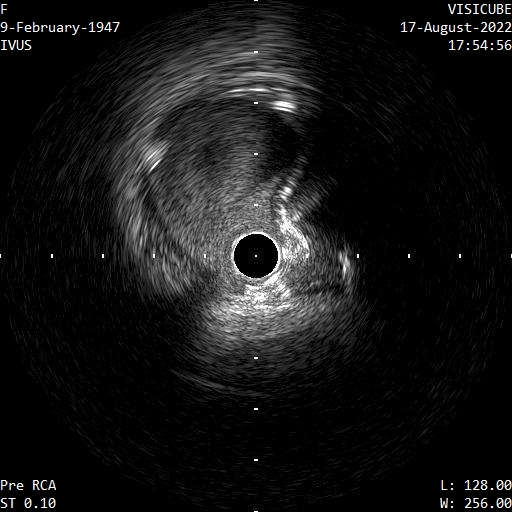
IVUS to RCA showed a calcium nodule at outer curve of proximal RCA causing in-stent restenosis.
Interventional Management
Procedural Step
A temporary pacing wire was placed into right ventricle through right femoral vein in the beginning.
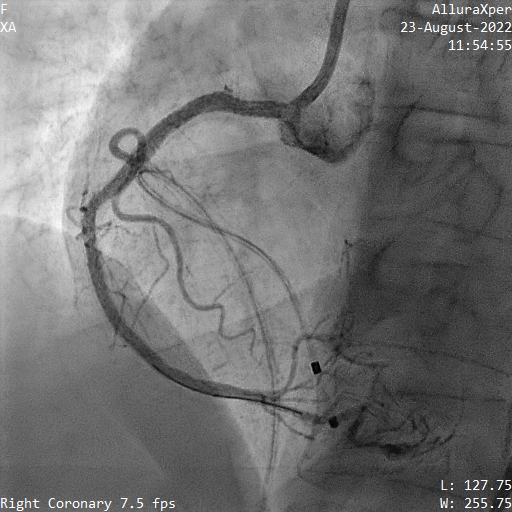
Ostial to proximal RCA was treated with 7 runs of RotaPro 2.0 burr. In traditional teaching rotablation could modify calcium at outer curve of a vessel. Yet in this case the stent strut on the calcium nodule was damaged as a result of the rotablation, as evidenced by IVUS. A 3.5mm non-compliant balloon was deployed at proximal RCA to flatten the disrupted stent strut. Ostial to proximal RCA was further treated with 3.5mm shockwave balloon for 8 cycles. Ostial to proximal RCA was stented with Xience Skypoint 3.5/15mm and post dilatation with non-compliant balloon was done. Final IVUS and angiogram showed acceptable result.
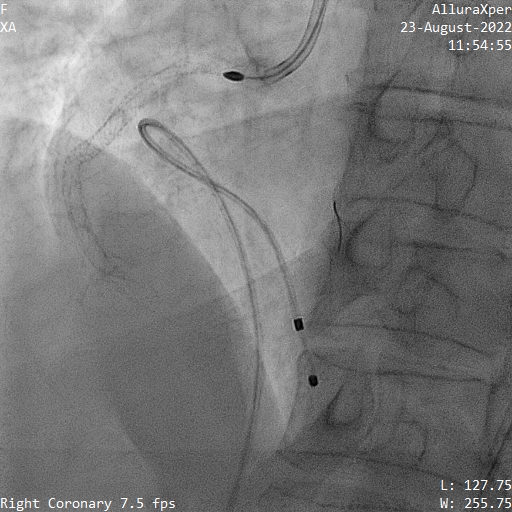

Ostial to proximal RCA was treated with 7 runs of RotaPro 2.0 burr. In traditional teaching rotablation could modify calcium at outer curve of a vessel. Yet in this case the stent strut on the calcium nodule was damaged as a result of the rotablation, as evidenced by IVUS. A 3.5mm non-compliant balloon was deployed at proximal RCA to flatten the disrupted stent strut. Ostial to proximal RCA was further treated with 3.5mm shockwave balloon for 8 cycles. Ostial to proximal RCA was stented with Xience Skypoint 3.5/15mm and post dilatation with non-compliant balloon was done. Final IVUS and angiogram showed acceptable result.
Case Summary
We described a case of in-stent restenosis caused by calcium nodule in which both rotablation and shockwave intravascular lithotripsy were done for calcium modification. This case highlighted the importance of pre-stenting imaging and adequate preparation of calcified lesion before stenting.