
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-107
From One Trap to Another - Dealing With a Fractured Microcatheter Tip
By Cliff Li, Fahim Jafary
Presenter
Cliff Li
Authors
Cliff Li1, Fahim Jafary1
Affiliation
Tan Tock Seng Hospital, Singapore1,
View Study Report
TCTAP C-107
CORONARY - Complications (Coronary)
From One Trap to Another - Dealing With a Fractured Microcatheter Tip
Cliff Li1, Fahim Jafary1
Tan Tock Seng Hospital, Singapore1,
Clinical Information
Patient initials or Identifier Number
OST
Relevant Clinical History and Physical Exam
A 57 year old male with a past medical history of diabetes mellitus, hyperlipidemia and prior history of CABG in 2009 (LIMA-LAD; SVG-RPDA; SVG-OM; SVG-D2) presented with new onset of chest pain. Clinical examination was unremarkable and vital signs stable.
Relevant Test Results Prior to Catheterization
Serial high-sensitivity troponin I was not raised and ECG shows no significant ST segment changes. Clinical impression was unstable angina and patient was counselled to undergo coronary angiogram (CAG).
Relevant Catheterization Findings
CAG shows severe native triple vessel disease; patent LIMA-LAD; severe disease in mid graft of SVG-RPDA and proximal-mid graft of SVG-D2; and occluded SVG-OM (stump seen). After discussion, it was decided to proceed with revascularisation. He underwent PCI to SVG-D2 with DES x2 (4.0 x 20mm; 3.5 x 48mm), followed by PCI to SVG-RPDA.
 211116 Broken MC tip - SVG RPDA AP Cr.Ser1.avi
211116 Broken MC tip - SVG RPDA AP Cr.Ser1.avi
211116 Broken MC tip - SVG-D 2 LAO Cr.avi
211116 Broken MC tip - PCI 1 - post PCI to SVG-D.Ser1.avi
Interventional Management
Procedural Step
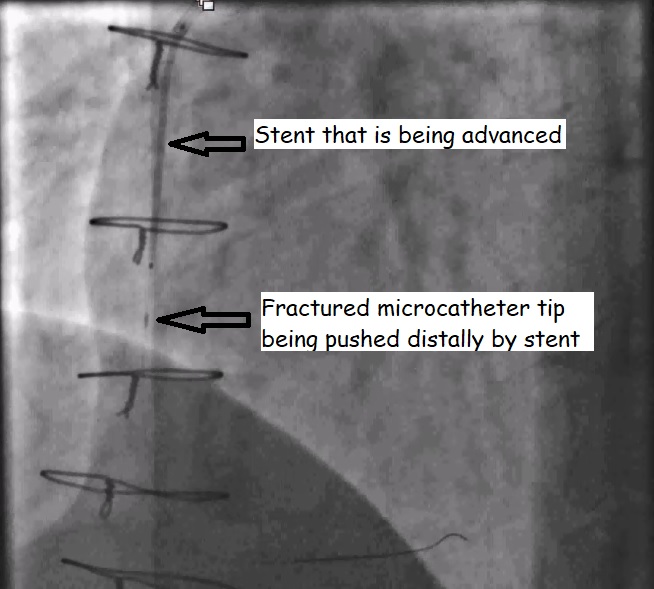
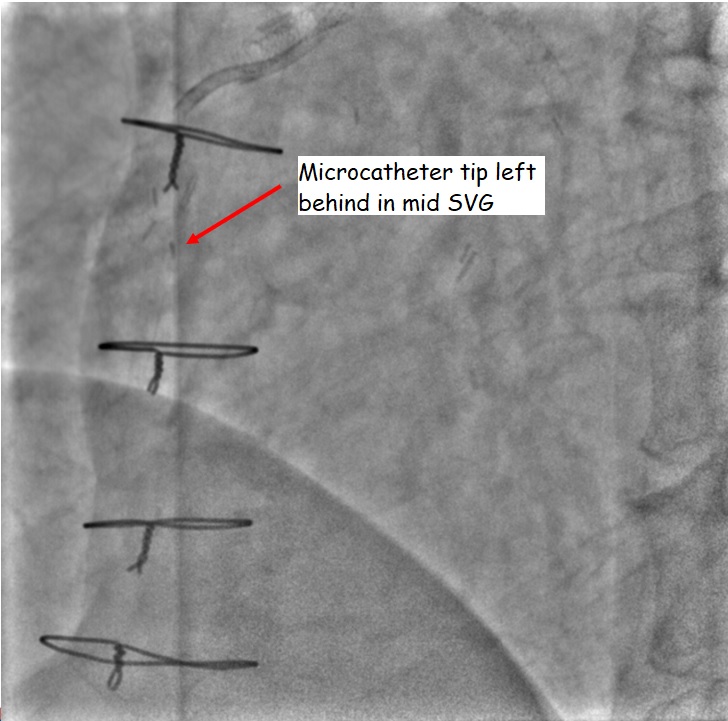
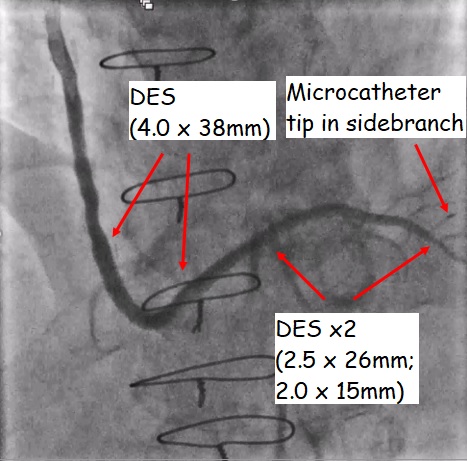
SVG-RPDA was engaged 6Fr AL1guiding catheter and Sion blue guidewire used to wire into distal SVG. IVUS shows fibro-calcific plaque in mid graft and hence was pre-dilated with a scoring balloon. Coronary slow flow ensued with TIMI 1 flow and ST elevation inleads III and aVF. Intracoronary adenosine and GTN were administered to distal coronary circulation via a microcatheter (MC) and re-established TIMI 3 flow. The MC was then removed after using Kusabi trapping balloon. Next, while advancing the DES into proximal SVG, a radiopaque object was noted distal to the stent markers. This is likely to be the MC tip that is fractured during the exchange and now being pushed distally by the stent. It was then realised that a 150cm MC was accidentally utilized instead of the usual 135cm length. The stent was removed immediately and 2 guidewires placed parallel, taking care not to push the MC tip further distally. These three guidewires were then slowly removed in a clockwise rotation but the tip slipped off the guidewire and was left in the mid SVG. Further attempts to snare the tip with Amplatz Goose Neck 4mm was unsuccessful. A 1.5 x 15mm balloon was unable to "trap" the tip and instead pushed it further down into RPDA. The tip eventually lodged within a small RPDA side branch and hence 2 stents were deployed from distal SVG to mid RPDA to secure the vessel and “trap” the tip in the side branch. Another stent was then placed in mid SVG to complete the procedure.
Case Summary
This case illustrates the different strategies that can be employed to deal with an embolised fractured microcatheter tip. A multi-guidewire technique followed by snaring strategy which failed, led to the deployment of the stents in main branch to "trap" the embolised microcatheter tip in a small side branch. It is important to have a calm and algorithmic approach to complications to ensure patient safety.