
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-079
Tip-in Technique for Dissected CTO of Lad Using Single Catheter
By Raghav Sharma
Presenter
Raghav Sharma
Authors
Raghav Sharma1
Affiliation
RKM Hospital, India1,
View Study Report
TCTAP C-079
CORONARY - Chronic Total Occlusion
Tip-in Technique for Dissected CTO of Lad Using Single Catheter
Raghav Sharma1
RKM Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Mr.PK
Relevant Clinical History and Physical Exam
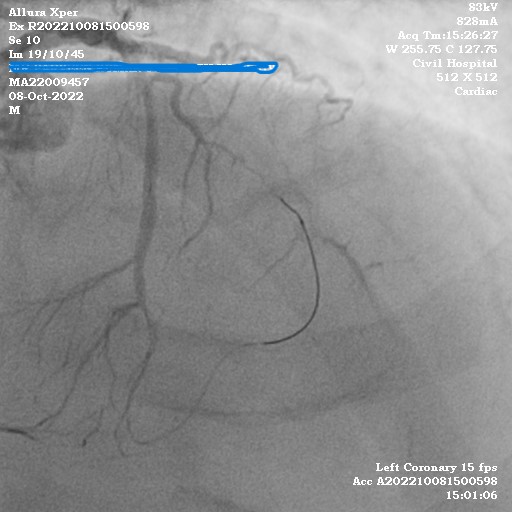
37 year old male presented with angina on exertion. CCS Class III. Patient is chronic smoker, hypertensive as well as non-diabetic. Electrocardiography was normal and their was no regional wall motion abnormality. With left ventricular ejection fraction of 50%.Coronary angiogram showed
LM normal
LAD 100% occluded from mid segment and filling retrogradely by homogenous collateral from septal LCX 100% occluded proximally non dominant vessel
RCA mid segment 99 percent stenosis dominant vessel.
LM normal
LAD 100% occluded from mid segment and filling retrogradely by homogenous collateral from septal LCX 100% occluded proximally non dominant vessel
RCA mid segment 99 percent stenosis dominant vessel.
Relevant Test Results Prior to Catheterization
echocardiography was normal and EKG showed no changes
Relevant Catheterization Findings
LM- 50% stenosis
LAD- Mid 100% CTO filling retrograde by septal collaterals and RCA
LCx- Proximal 100% CTO
RCA- Mid 99% concentric focal stenosis



LAD- Mid 100% CTO filling retrograde by septal collaterals and RCA
LCx- Proximal 100% CTO
RCA- Mid 99% concentric focal stenosis
Interventional Management
Procedural Step
Angioplasty-
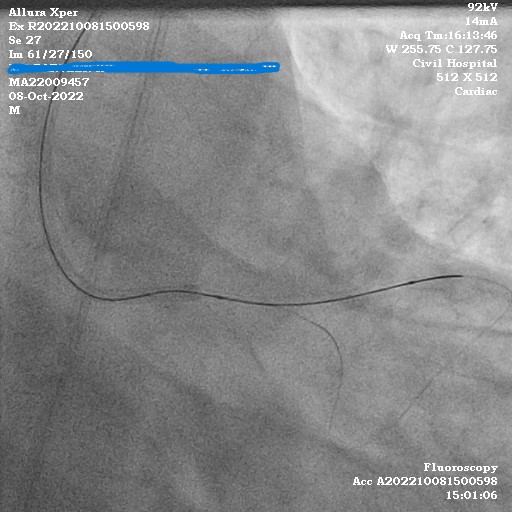
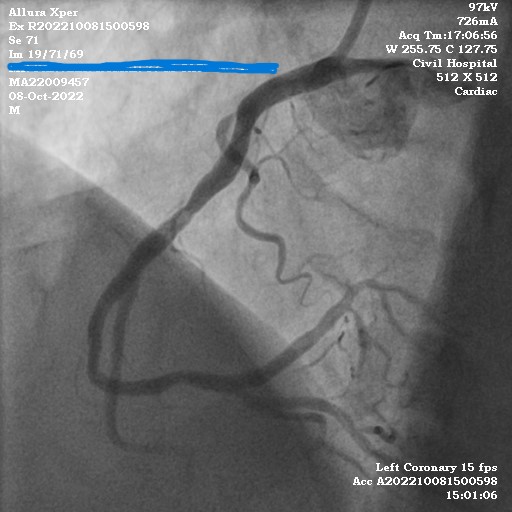
Case Summary
Retrograde using single catheter via homogenous collateral poses greater challenge. In this case it was difficult to push in micro catheter into same guide, hence tip-in technique was used where antegrade micro catheter was parked over the retrograde wire and then it was parked in mid LAD and antegrade wire was taken. Tip-in is an excellent technique requiring correct understanding of branch, angle of guide and poses a great technical challenged.