
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-149
A Case Report of Class II Endovenous Heat-Induced Thrombosis Post Endovenous Laser Ablation: Prompt Treatment or Watchful Waiting?
By Ifan Citra, Fery Budiman Santoso, Vekky Sariowan, Janry Antonius Pangemanan, Agnes Lucia Panda
Presenter
Ifan Citra
Authors
Ifan Citra1, Fery Budiman Santoso2, Vekky Sariowan3, Janry Antonius Pangemanan2, Agnes Lucia Panda3
Affiliation
Mitra Keluarga Kelapa Gading Hospital, Indonesia1, RSUP Prof Dr RD Kandou Manado, Indonesia2, Sam Ratulangi University Manado, Indonesia3,
View Study Report
TCTAP C-149
ENDOVASCULAR - Peripheral Vascular Disease and Intervention
A Case Report of Class II Endovenous Heat-Induced Thrombosis Post Endovenous Laser Ablation: Prompt Treatment or Watchful Waiting?
Ifan Citra1, Fery Budiman Santoso2, Vekky Sariowan3, Janry Antonius Pangemanan2, Agnes Lucia Panda3
Mitra Keluarga Kelapa Gading Hospital, Indonesia1, RSUP Prof Dr RD Kandou Manado, Indonesia2, Sam Ratulangi University Manado, Indonesia3,
Clinical Information
Patient initials or Identifier Number
YM
Relevant Clinical History and Physical Exam
A 78-year-old woman came to clinic with a major complaint of pain in the left lower limb since 5 years ago. She had a history of hypertension, no smoking habit, and no history of thromboembolic or cardiovascular event. On admission, the patient was overweight with BMI of 27.3 kg/m2 and blood pressure was 144/84 mmHg. The left limb had varicose veins extended to the thigh, accompanied by diffuse lipodermatosclerosis on lower third calf.

Relevant Test Results Prior to Catheterization
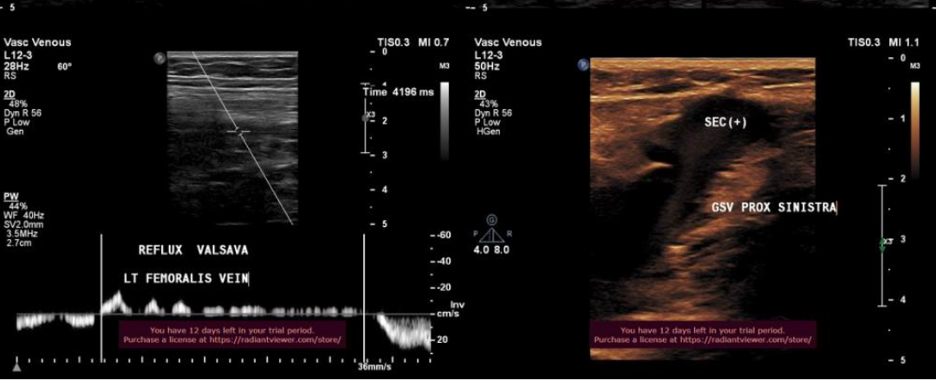
Duplex ultrasound (DUS) in the left limb showed spontaneous echo contrast in upper knee great saphenous vein (GSV). The left femoral vein had spontaneous reflux and significant reflux during Valsava maneuver with reflux time >4000 ms. Ankle brachial index was 1.2 in the left limb. Electrocardiogram showed first-degree AV block with ventricular rate of 68 bpm. The patient was diagnosed with stage C4 severe chronic venous insufficiency (CVI).
Relevant Catheterization Findings
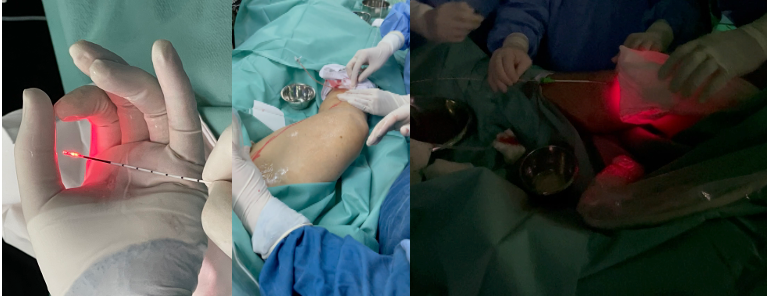
Endovenous Laser Ablation (EVLA) was performed with DUS guidance. Puncture was performed in below knee left GSV and a laser catheter was inserted with catheter tip placed 2 centimeters from the junction. Cold tumescent at 50 Celsius with saline solution was injected into the patient. Ablation was conducted with 1,470 nm laser power set at 10 Watt, linear endovenous energy density (LEED) 70 Joule/cm and pullback velocity 1.5 mm/s. A sterile ice pack was applied immediately after ablation.
Interventional Management
Procedural Step
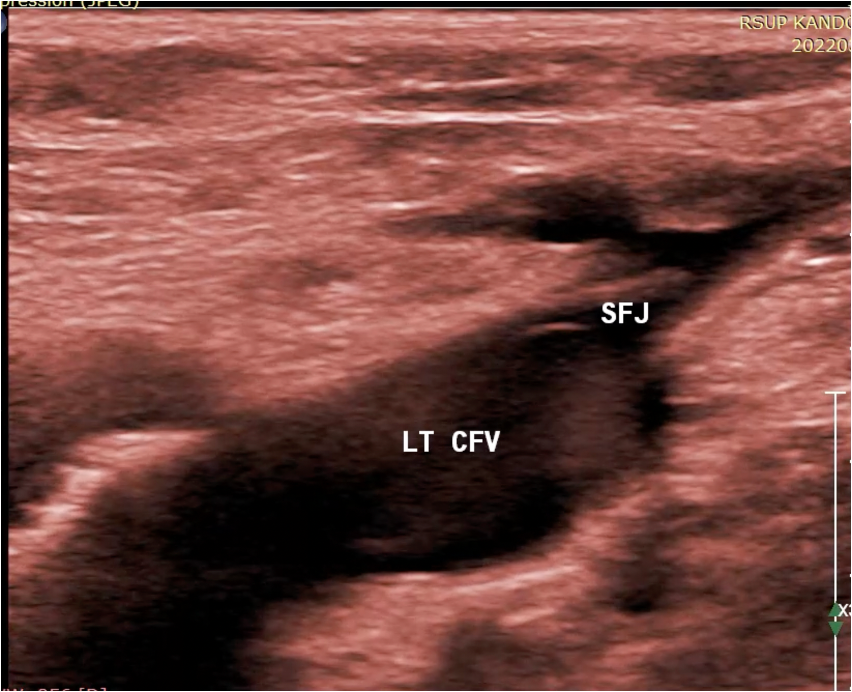
After the procedure, DUS surveillance showed GSV was obliterated and soon after, compression stocking was applied. The patient was only given paracetamol to relieve pain. Two days after the procedure, there was a thrombus in the proximal left upper knee GSV with propagation into common femoral vein that comprised <50% lumen. The patient was diagnosed with class II endovenous heat-induced thrombosis (EHIT II American Venous Forum classification system). The patient only experienced mild pain in the left limb. Besides compression stocking, there was no further treatment given. After one week observation, the thrombus did not resolve. After one month post EVLA, the patient was asymptomatic. DUS surveillance showed significant thrombus reduction and she was diagnosed with EHIT I. There was not any additional treatment prescribed.


Case Summary
DUS surveillance should be done within one week after procedure to diagnose EHIT. Perioperative use of heparin and compression stocking after EVLA have been reported for EHIT prevention. An additional technique that could prevent EHIT is to place distal ablation catheter tip >2.5 cm from deep vein junction. Until now, there are conflicting data regarding treatment in EHIT II. Surveillance is an option for EHIT II. Nevertheless, in high-risk patients anticoagulation should be considered. This patient has mild symptoms with no thromboembolic history. Therefore, we decided to withhold anticoagulation. After one month of surveillance, thrombus regression was achieved without medication.