
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-095
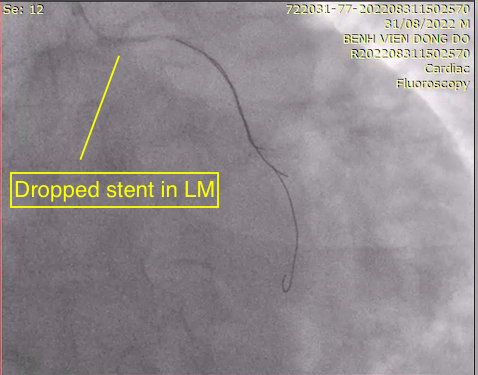
When Things ‘Falls’ off Hand: How to Save: In the Case of a Stent Loss in the Left Coronary Artery
By Quan Manh Nguyen, Tung Ngo, Pham Manh Hung
Presenter
Ngo Quang Tung
Authors
Quan Manh Nguyen1, Tung Ngo1, Pham Manh Hung1
Affiliation
Vietnam National Heart Institute, Vietnam1,
View Study Report
TCTAP C-095
CORONARY - Complications (Coronary)
When Things ‘Falls’ off Hand: How to Save: In the Case of a Stent Loss in the Left Coronary Artery
Quan Manh Nguyen1, Tung Ngo1, Pham Manh Hung1
Vietnam National Heart Institute, Vietnam1,
Clinical Information
Patient initials or Identifier Number
N.K.C
Relevant Clinical History and Physical Exam
41-year-old male patient
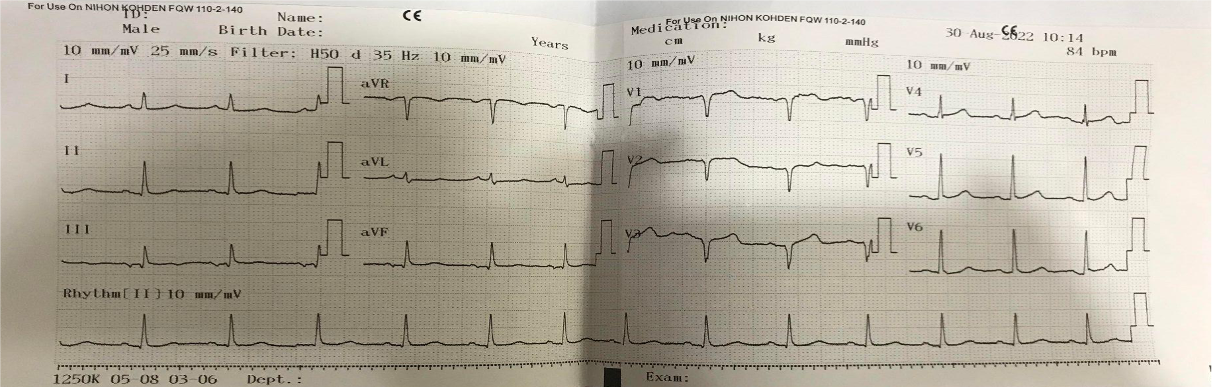
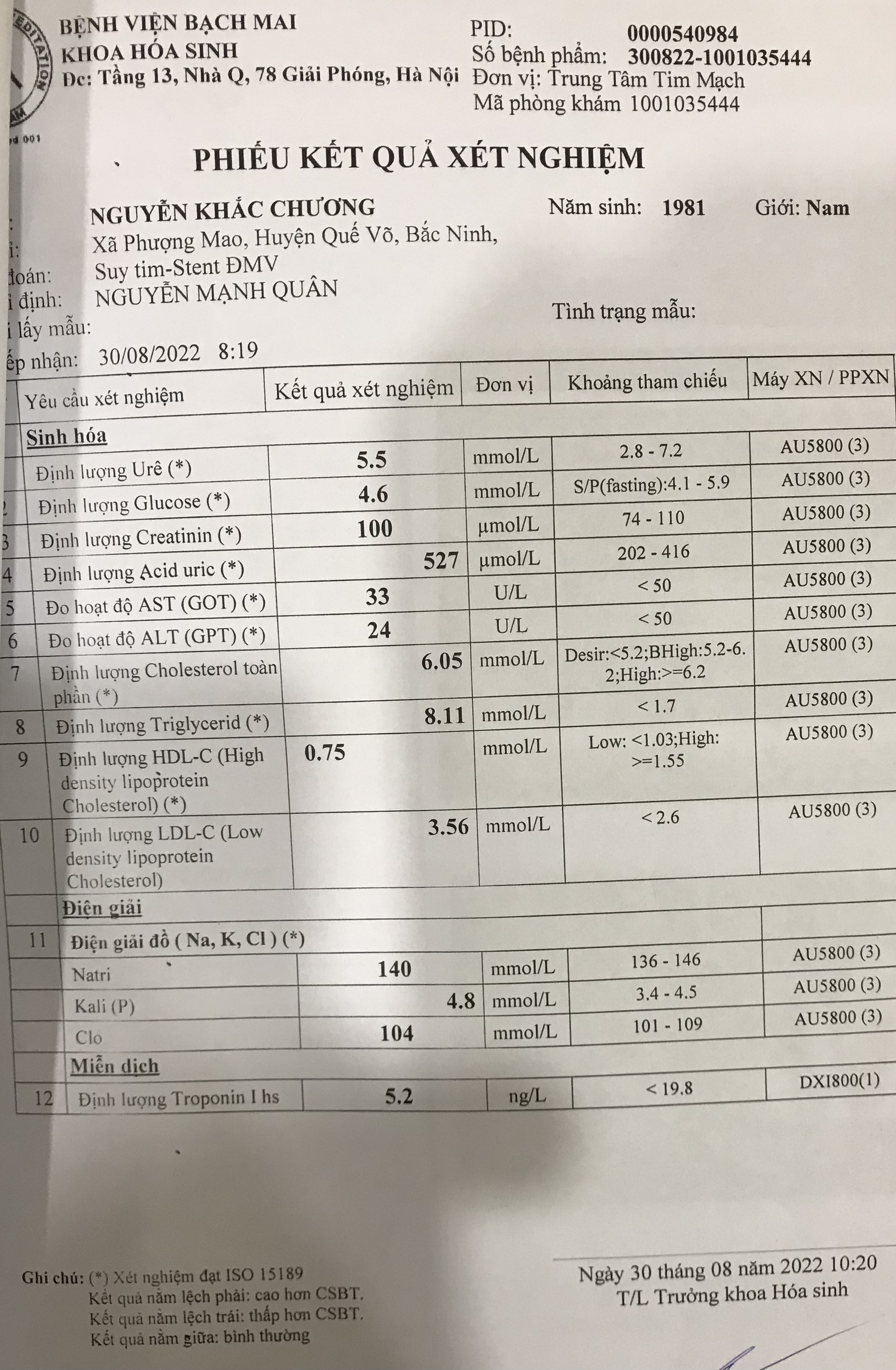
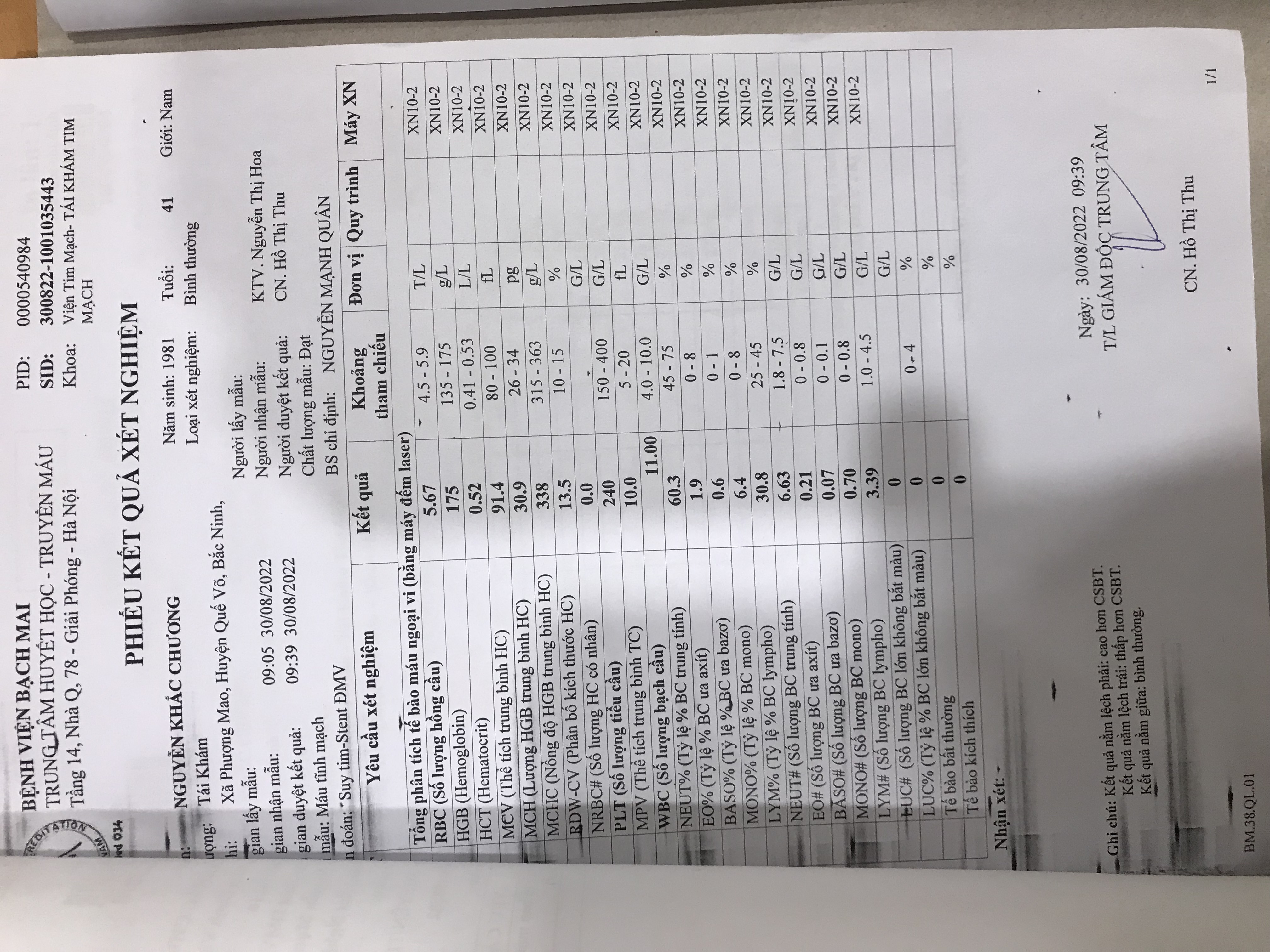
Relevant Test Results Prior to Catheterization
- CBC: Hb 17.5 g/dl ( 13.5 - 17.5 g/dl ) ; PLT 240 G/L ( 150 - 400 G/L)
Relevant Catheterization Findings
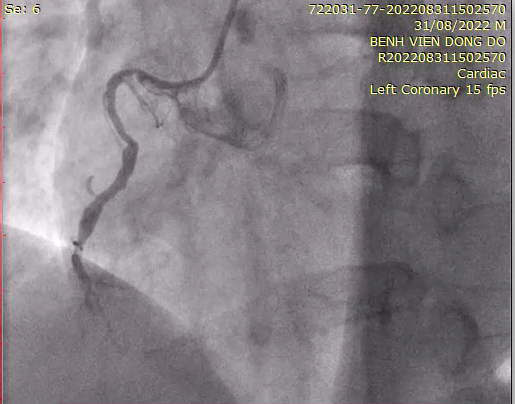
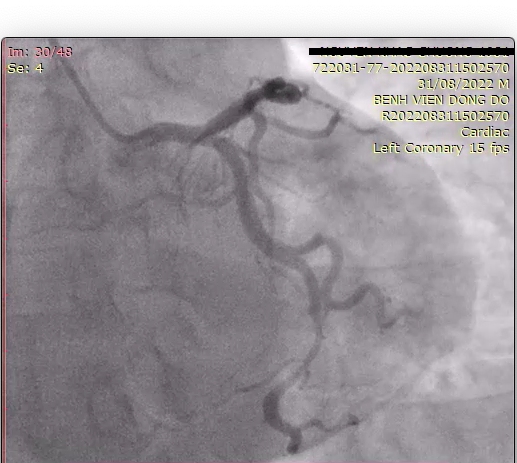
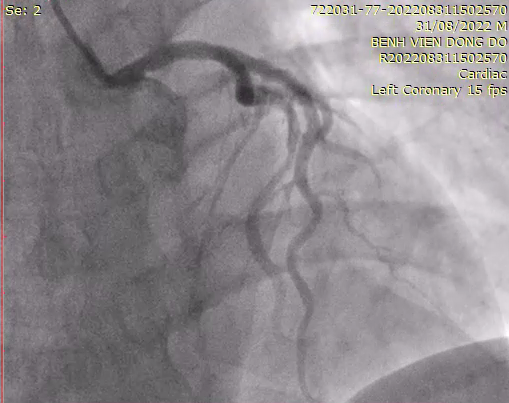
- The proximal-middle LAD stent still has a good flow. 80-85% stenosis in the middle of LCX. There is a previous stent in the proximal of LCX
Interventional Management
Procedural Step
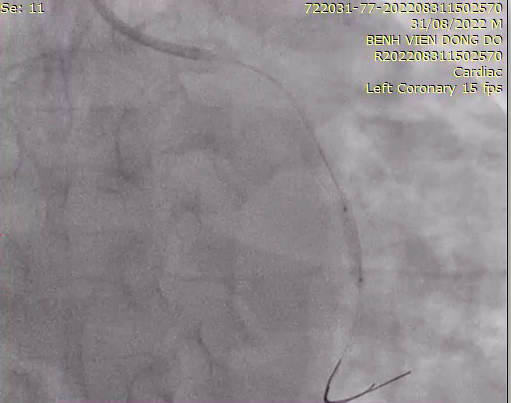
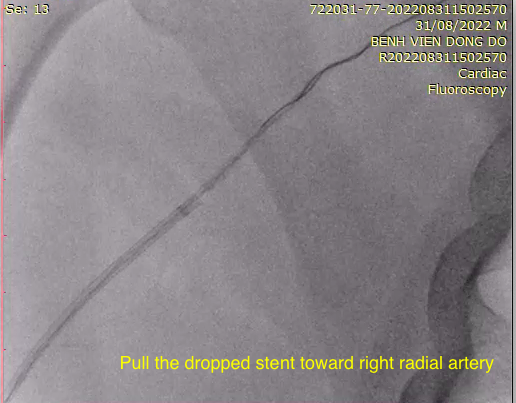
We use access: Right radial artery; Introducer: 6F; Guiding catheter: EBU, 6F; Guidewire: Runthrough and Predilatation with 2.5x20 mmm balloon. However, we failed to deliver the stent into the mLCX through the previous stent in pLCX.
Case Summary
· Stent loss is not an exceptional complication of percutaneous coronary intervention and can be life-threatening.