
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-201
Optimal Implantation Depth of a Self-Expandable TAVR Device in a Patient With Type 0 Bicuspid Aortic Valve With Severe Stenosis and Calcification Guided by In-Silico Simulation
By Xinlei Wu, Patrick W. Serruys, Xiaojie Yu, Yuanxue Sun, Yanru Chen, Daozhu Wu, Xinmin Zhang, Lianpin Wu
Presenter
Xinlei Wu
Authors
Xinlei Wu1, Patrick W. Serruys2, Xiaojie Yu3, Yuanxue Sun3, Yanru Chen3, Daozhu Wu1, Xinmin Zhang1, Lianpin Wu1
Affiliation
The Second Affiliated Hospital of Wenzhou Medical University, China1, University of Galway, Ireland2, Second Affiliated Hospital Wenzhou Medical University, China3,
View Study Report
TCTAP C-201
STRUCTURAL HEART DISEASE - Valvular Intervention: Aortic
Optimal Implantation Depth of a Self-Expandable TAVR Device in a Patient With Type 0 Bicuspid Aortic Valve With Severe Stenosis and Calcification Guided by In-Silico Simulation
Xinlei Wu1, Patrick W. Serruys2, Xiaojie Yu3, Yuanxue Sun3, Yanru Chen3, Daozhu Wu1, Xinmin Zhang1, Lianpin Wu1
The Second Affiliated Hospital of Wenzhou Medical University, China1, University of Galway, Ireland2, Second Affiliated Hospital Wenzhou Medical University, China3,
Clinical Information
Patient initials or Identifier Number
02244321
Relevant Clinical History and Physical Exam
A 74-year-old man (Height: 166cm, Weight: 68.2kg, BMI: 24.7) with a history of percutaneous coronary intervention six years ago was referred to our hospital with sudden syncope and urinary incontinence (NYHA class II). Transthoracic echocardiography (TTE) revealed that he was type 0 bicuspid aortic valve (BAV) with heavy calcification, severe stenosis, and mild insufficiency (mean pressure gradient: 46 mmHg, valve orifice area: 0.46 cm2, and ejection fraction: 53%).
Relevant Test Results Prior to Catheterization
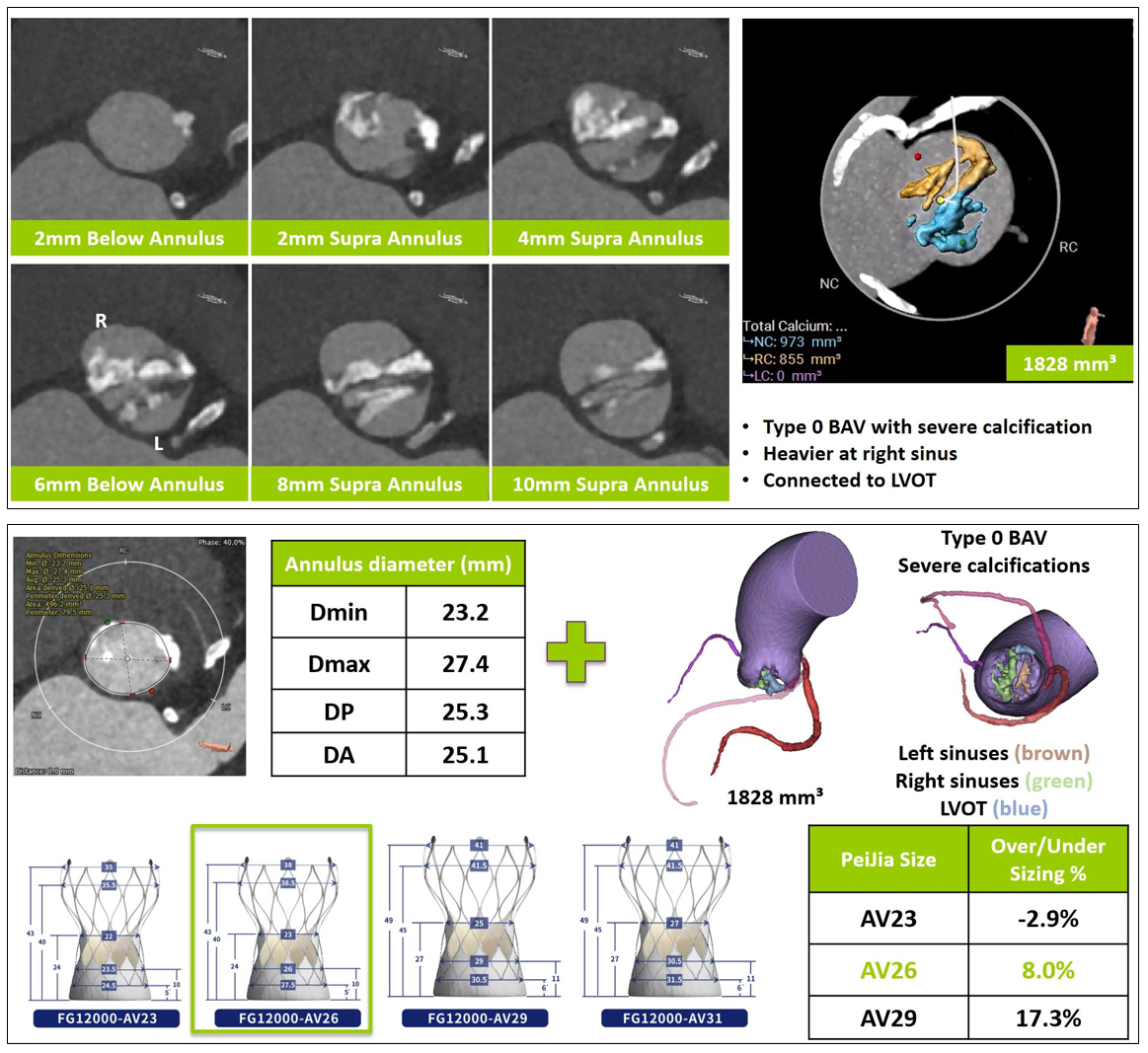
CCTA confirmed that this is a case of type 0 BAV with severe stenosis and calcification, especially on the leaflet in right coronary sinus (Figure 1). The diameter of RCA ostium is only 0.9mm. The min and max diameters at the levels of LVOT (below 5mm annulus), annulus, SOV, STJ, and enlarged AA (above 40mm annulus) are 21.5X29.0mm, 23.2X27.4mm, 28.7X36.8mm, 35.5X36.5mm, 45.6X46.8mm, respectively. The height of both coronary ostia are 15.7 and 17.1mm. The atrioventricular angle is 57°.
Relevant Catheterization Findings
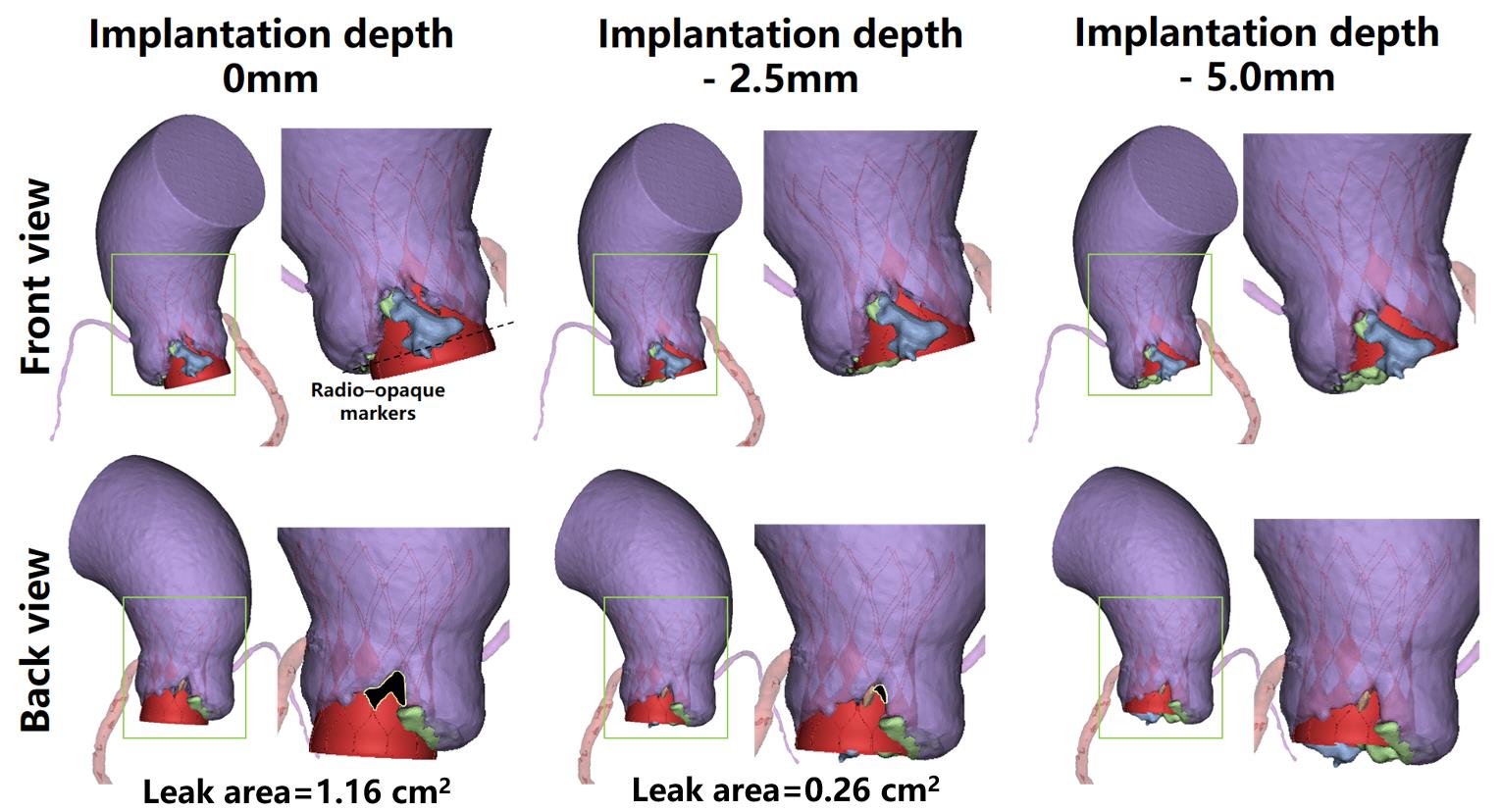
The severe calcification was connected to LVOT with a volume of 1828mm3. Based on the averaged diameters of the annulus (25mm) and the heavy calcification of BAV, AV26 was only chosen with an oversizing 8.0% (Figure 1). The three different implantation depth of the device was tested by in-silico simulation at 0mm, -2.5mm, and -5mm. And it was found that the implantation depth (0 or -2.5mm) had intervalvular leak areas with 1.16, and 0.26cm2, whereas the depth (-5mm) could block well (Figure 2).
Interventional Management
Procedural Step
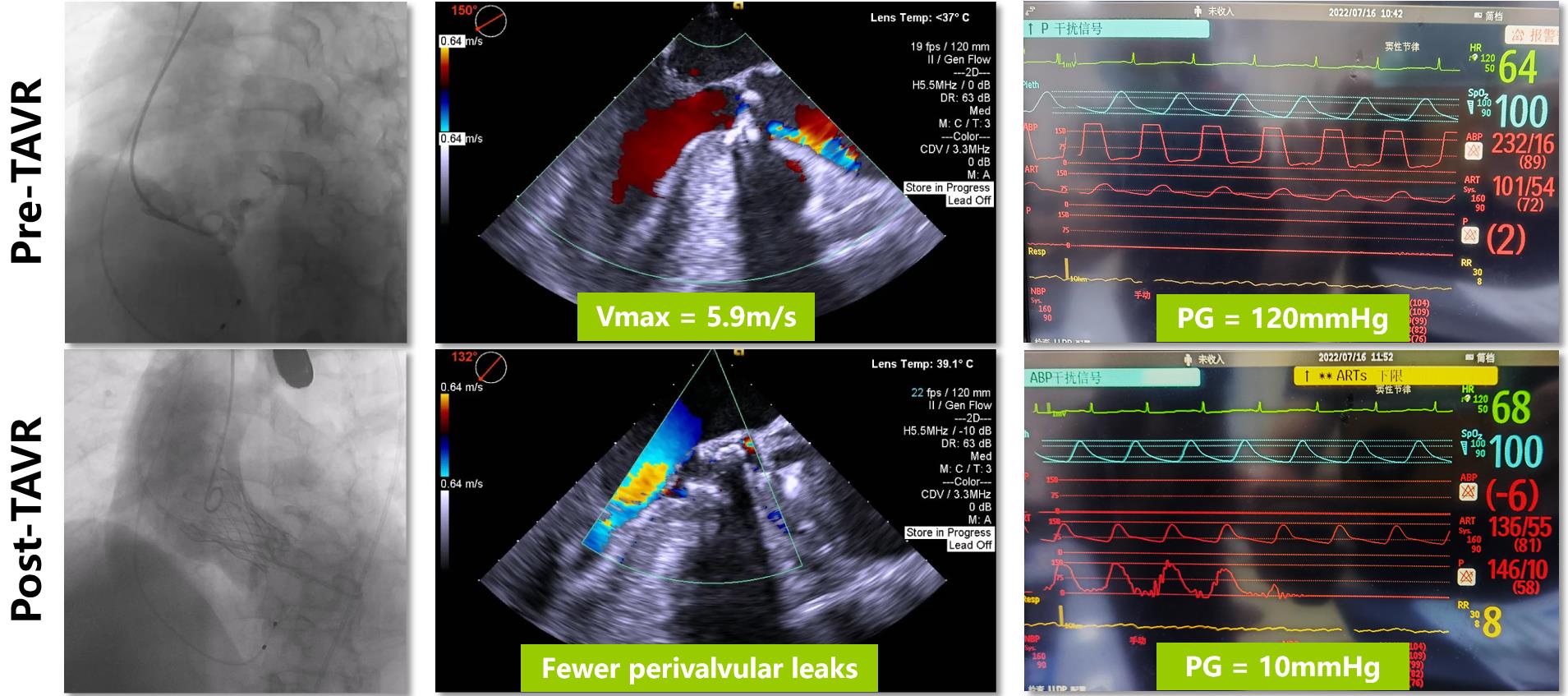
After general anesthesia, the main approach was established at the right femoral artery with a lumen diameter of 8.8 mm. Then, angiography showed that the leaflets had severe calcification with very poor mobility (Figure 3 Top left). A 20 mm × 50 mm balloon was used to pre-dilate the native valves. “Waist sign” above the annulus during aortic valvuloplasty was clearly observed. It further confirmed that the size of the prosthesis should be "downsizing" and selected AV26. However, the pre-dilatated balloon suddenly ruptured at nominal pressure, which might be caused by severe calcification. Meanwhile, the patient's vital signs remained stable. Afterward, the ruptured balloon was removed with the sheath. In order to avoid the tear risk of the severely dilated ascending aorta(maximum diameter: 52.6mm), the prosthesis was carefully pulled using a snare at the central path of the lumen. According to the preoperative strategy suggested by the in-silicon simulation, the prosthesis was delivered to the location of 5mm above the aortic annulus and swiftly released to the working position. Transesophageal echocardiography confirmed that the prosthesis was steadily anchored with mild regurgitation. The prosthesis was carefully fully released. The post-dilatation balloon was performed to improve the shape of the prosthesis. Finally, the peak pressure gradient dramatically decreased from 120 mmHg to 10 mmHg after TAVR (Figure 3 Bottom Right).
Case Summary
The optimal implantation depth of this type 0 BAV is appropriate high above the annulus to avoid leakage from intervavular triangle. Pre-procedural CT assessment is crucial to plan the optimal individual treatment for high-risk patients with BAV with severe stenosis and calcification. In-silico simulation could be a useful method to provide the direct observation of the interaction between the prosthesis and aortic root complex prior to TAVR, and help to accurate assessment for the optimal treatment of high-risk patients.