
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-002
An Uncommon Masquarade of Inferior STEMI
By Lung En Teng, Saadat Ali Saleemi, Nay Min Htun
Presenter
Lung En Teng
Authors
Lung En Teng1, Saadat Ali Saleemi2, Nay Min Htun3
Affiliation
Peninsula Health, Australia1, Epworth Hospital, Australia2, Alfred Hospital, Australia3,
View Study Report
TCTAP C-002
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
An Uncommon Masquarade of Inferior STEMI
Lung En Teng1, Saadat Ali Saleemi2, Nay Min Htun3
Peninsula Health, Australia1, Epworth Hospital, Australia2, Alfred Hospital, Australia3,
Clinical Information
Patient initials or Identifier Number
GS
Relevant Clinical History and Physical Exam
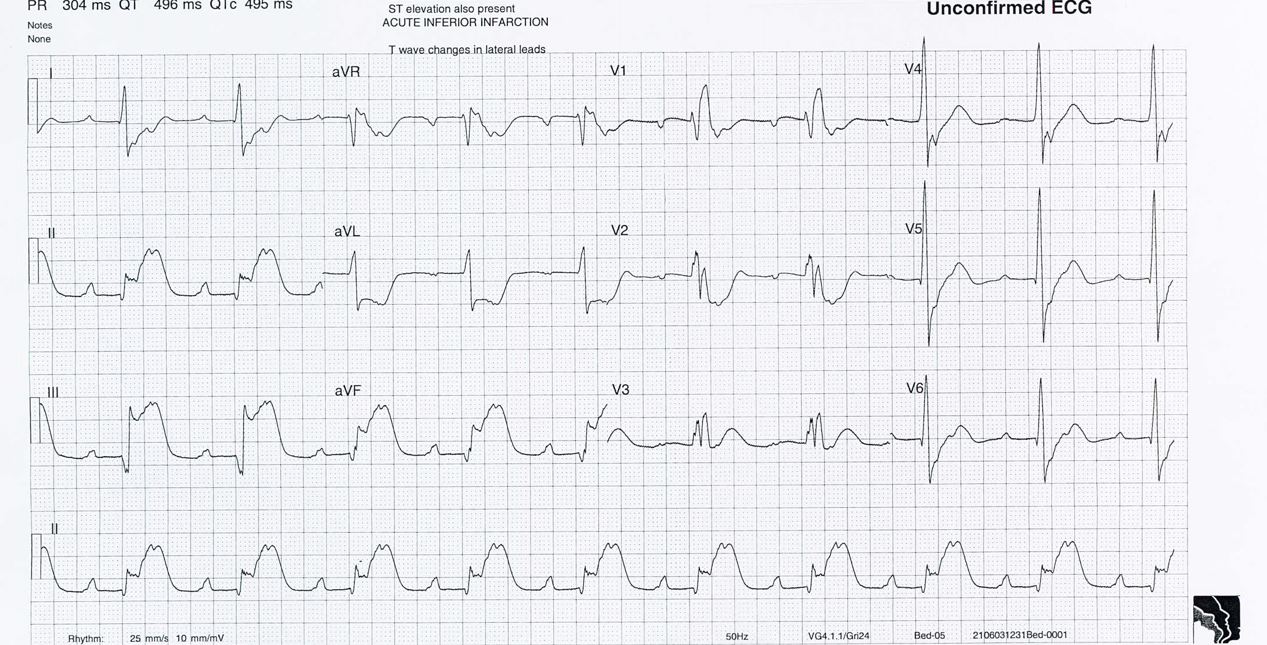
54 year old male was brought into emergency department with chest pain as ST Elevation Myocardial Infarction (STEMI) alert. He had a background history of hypertension. He complained of chest pain the evening before which got worse the next day. His vitals were: BP 164/86, oxygen sats 94% on room air, HR 66/min and RR 20/min. His chest was clear to auscultation and his heart sound was dual with no murmur. His ECG showed inferior STEMI. He was loaded with 300mg of aspirin by the paramedics crew.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
Patient was transferred urgently to the catheterization lab. Ultrasound guided vascular access was obtained in the right femoral artery. JL-4 Catheter was used but noted to be catching in the ascending aorta. JR-4 guide into aortic root withnon-selective shot suggesting aortic dissection - filling the right coronary artery therefore in the false lumen. This is then confirmed with pigtail aortogram where the true lumen is shown and filling the left main artery.


Case Summary
In conclusion, clinicians need to have a high index of suspicion for aortic dissection in patients with chest pain. Myocardial infarction resulted from functional coronary artery occlusion where the dissection flap occluded the ostium of right coronary artery. Prompt diagnosis could avoid unnecessary anticoagulation that may result in fatal outcomes.