
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-041
Shocking Away Cardiogenic Shock
By David Yong, Jayakhanthan Kolanthaivelu
Presenter
David Yong
Authors
David Yong1, Jayakhanthan Kolanthaivelu2
Affiliation
National Heart Institute, Malaysia1, Cardiovascular Sentral Kuala Lumpur, Malaysia2,
View Study Report
TCTAP C-041
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Shocking Away Cardiogenic Shock
David Yong1, Jayakhanthan Kolanthaivelu2
National Heart Institute, Malaysia1, Cardiovascular Sentral Kuala Lumpur, Malaysia2,
Clinical Information
Patient initials or Identifier Number
LHS
Relevant Clinical History and Physical Exam
58 year old gentleman presented with sudden onset central chest pain. He was diagnosed with Acute Anterior Myocardial Infarction. At presentation he was hypotensive with BP 80/40mmHg and required ionotropic support with IVI norepinephrine. Proceeded with primary percutaneous intervention.
Relevant Test Results Prior to Catheterization
ECG showed ST elevation over anterior leads.
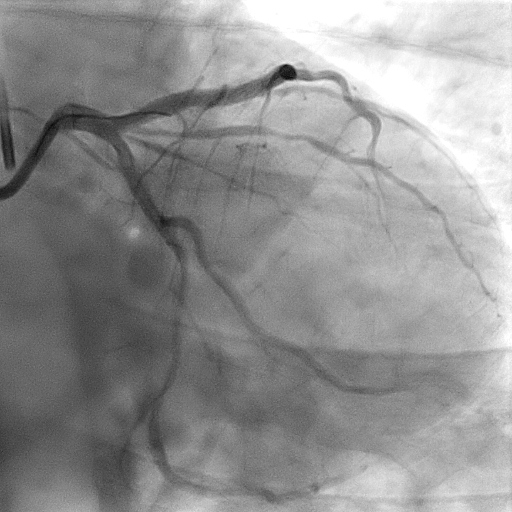
Relevant Catheterization Findings
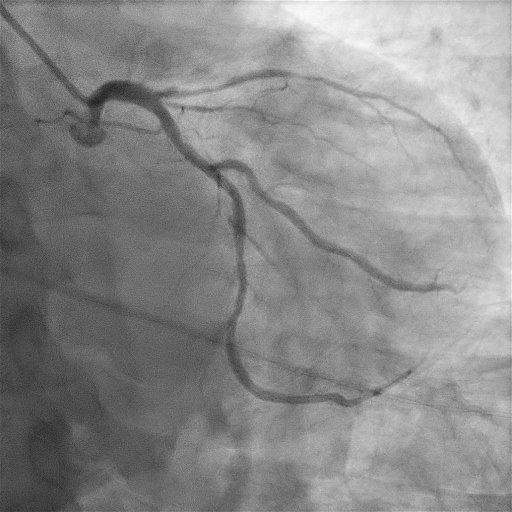
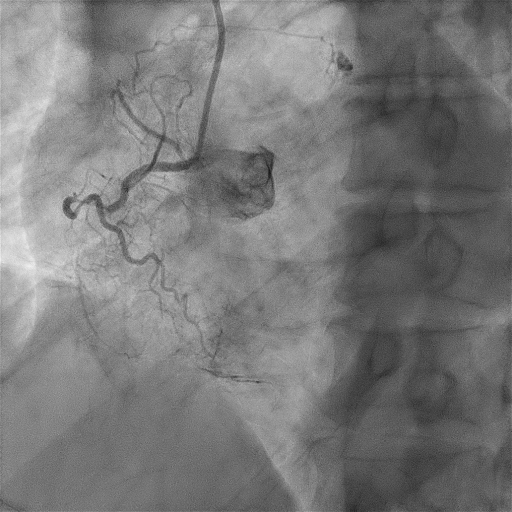
Coronary angiogram performed showed acute total occlusion of proximal left anterior descending artery with severe calcification and chronic total occlusion at proximal right coronary artery. Balloon angioplasty performed to proximal left anterior descending but unable to dilate fully. Flow was established and procedure stopped. Intra-aortic balloon pump inserted for circulatory support.
Interventional Management
Procedural Step
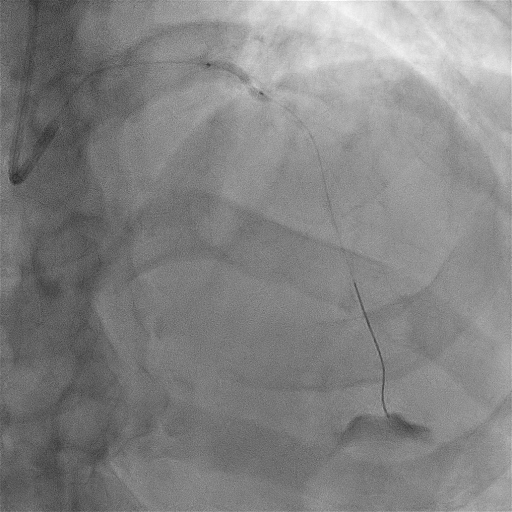
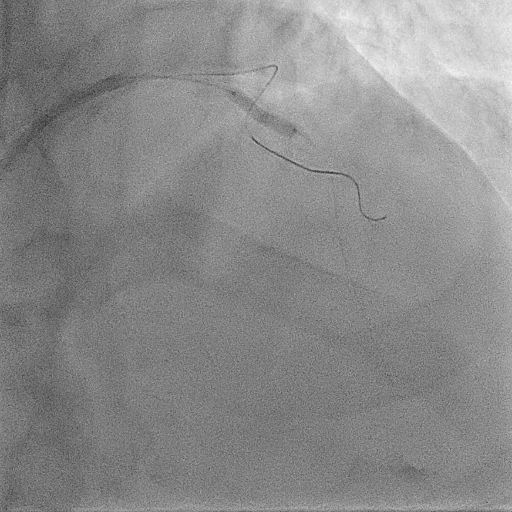
In view of persistent chest pain and unable to wean off ionotropes, decided to proceed with angioplasty the following day with plaque modificaton. Intravascular ultrasound (IVUS) perfomed showed severe calcification at proximal LAD. Proceed with scoring balloon 2.5/15 at high pressure up to 24atm. Intravascular lithotripsy performed with 3.0/12 balloon. Delivered total 80 shocks. IVUS repeated showed significant cracks. Stented with drug eluting stent 3.0/48. Post dilated proximal LAD with NC 3.5/15. IVUS showed good stent apposition and expansion. TIMI III flow angiographically. Throughout procedure, hemodynamics remained stable with no significant hypotensive episodes.

Case Summary
Post procedure, chest pain resolved. Patient was able to wean off IABP and ionotropes the following day. He was discharged well. Balloon undilatable lesion are often due to heavily calcified plaques. Intravascular lithrotripsy would make a good option in patients with cardiogenic shock as it avoids the risk of slow flow common in arthrectomy procedures such as rotablation which could possibly worsen the hemodynamic instability.