
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-205
Acute Papillary Muscle Rupture With Torrential Mitral Regurgitation: The Role of PASCAL in Haemodynamic Stabilisation
By Hashrul Rashid, Bernard Prendergast, Simon Redwood, Tiffany Patterson
Presenter
Hashrul Rashid
Authors
Hashrul Rashid1, Bernard Prendergast2, Simon Redwood2, Tiffany Patterson2
Affiliation
Monash University, Australia1, St Thomas’ Hospital, United Kingdom2,
View Study Report
TCTAP C-205
STRUCTURAL HEART DISEASE - Valvular Intervention: Mitral or Tricuspid
Acute Papillary Muscle Rupture With Torrential Mitral Regurgitation: The Role of PASCAL in Haemodynamic Stabilisation
Hashrul Rashid1, Bernard Prendergast2, Simon Redwood2, Tiffany Patterson2
Monash University, Australia1, St Thomas’ Hospital, United Kingdom2,
Clinical Information
Patient initials or Identifier Number
AB
Relevant Clinical History and Physical Exam
55M with torrential MR and ruptured papillary muscle on VA-ECMO transferred to our centre. At referring hospital, had late LCx stent thrombosis and torrential MR. PCI to LCx complicated by LMCA dissection, treated with LMCA, LAD and LCx stents. IABP and later VA-ECMO inserted due to cardiogenic shock. Initially referred for MV surgery, but due to extremis, referred to cardiology team.
Apologies, I could not include the video due to trouble with downloading the video from the hospital system.
Apologies, I could not include the video due to trouble with downloading the video from the hospital system.
Relevant Test Results Prior to Catheterization
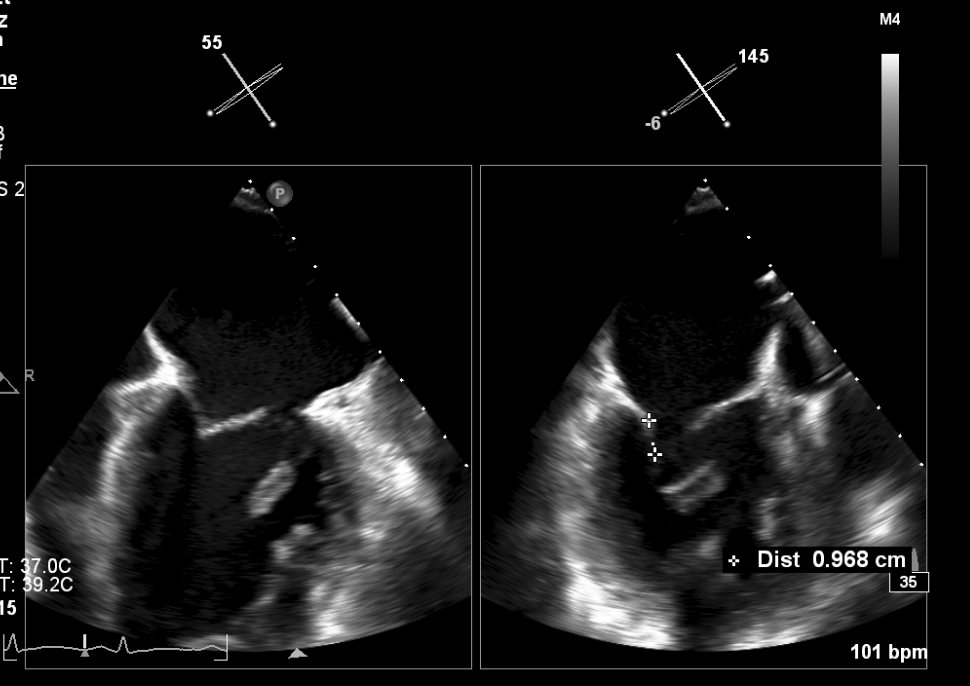
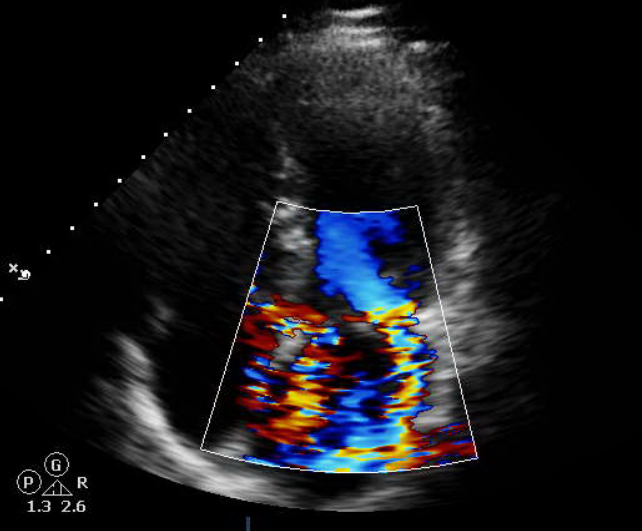
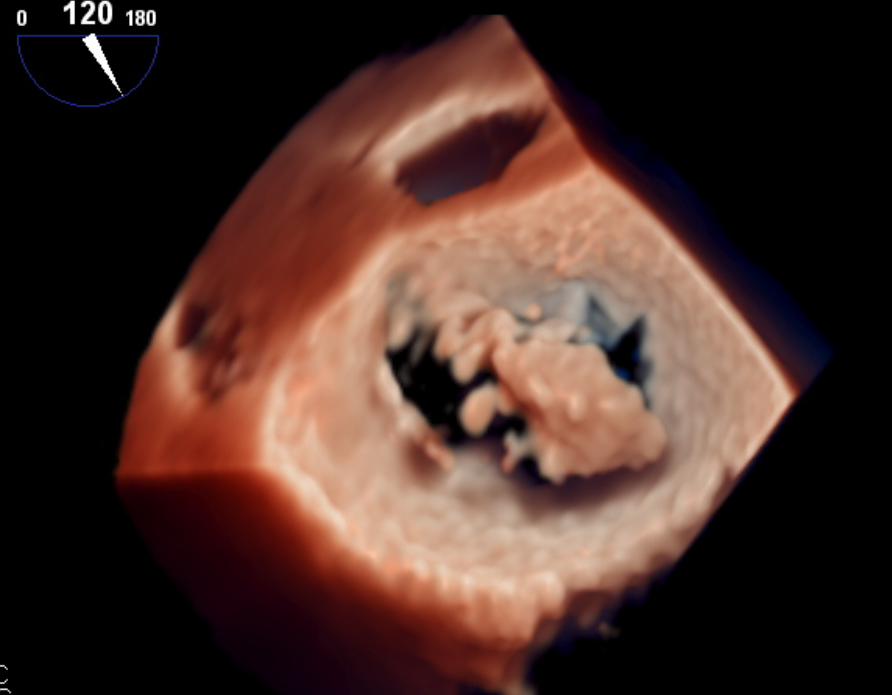
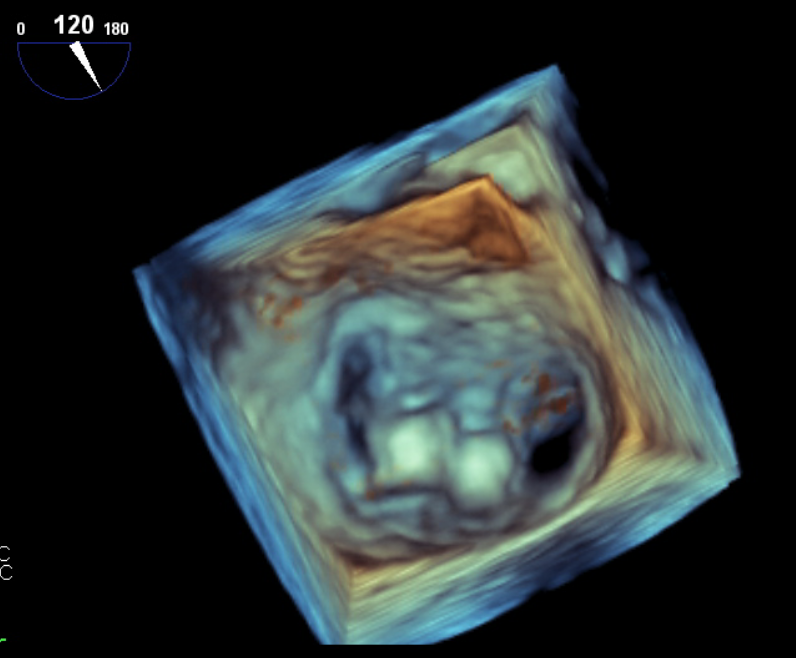
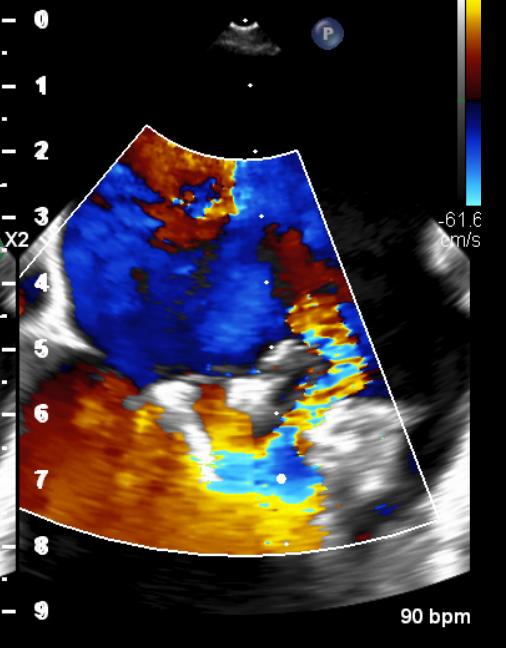
TTE: Ruptured anterior papillary muscle and torrential MR.
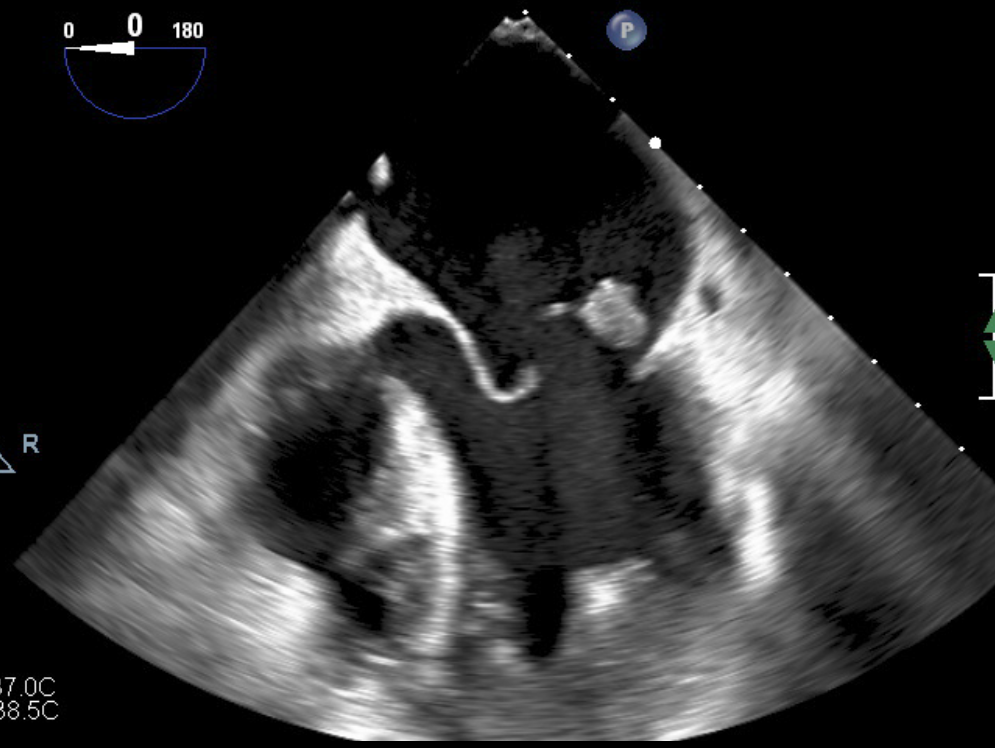
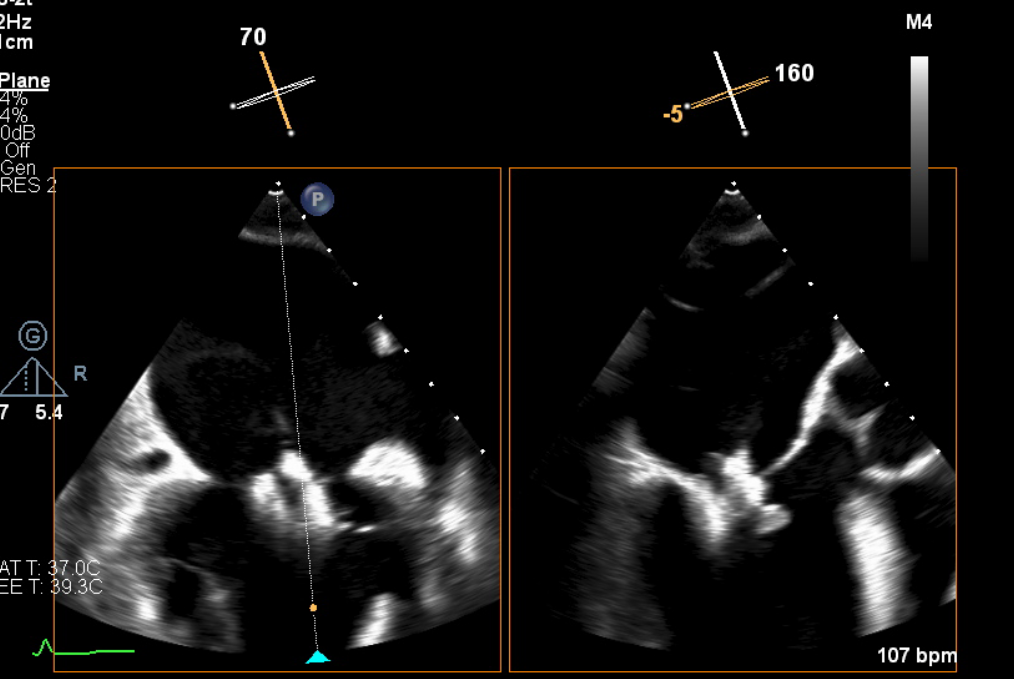
TOE: Torrential MR. There was flail anterior leaflet, constant movement of the papillary muscle with multiple subvalvular papillary chords. The posterior leaflet was restricted. The left atrial size was small (due to acute MR), which may prove challenging for transeptal puncture height.
Apologies, I was unable to include the video due to trouble with downloading video from the hospital system, will include in final presentation.
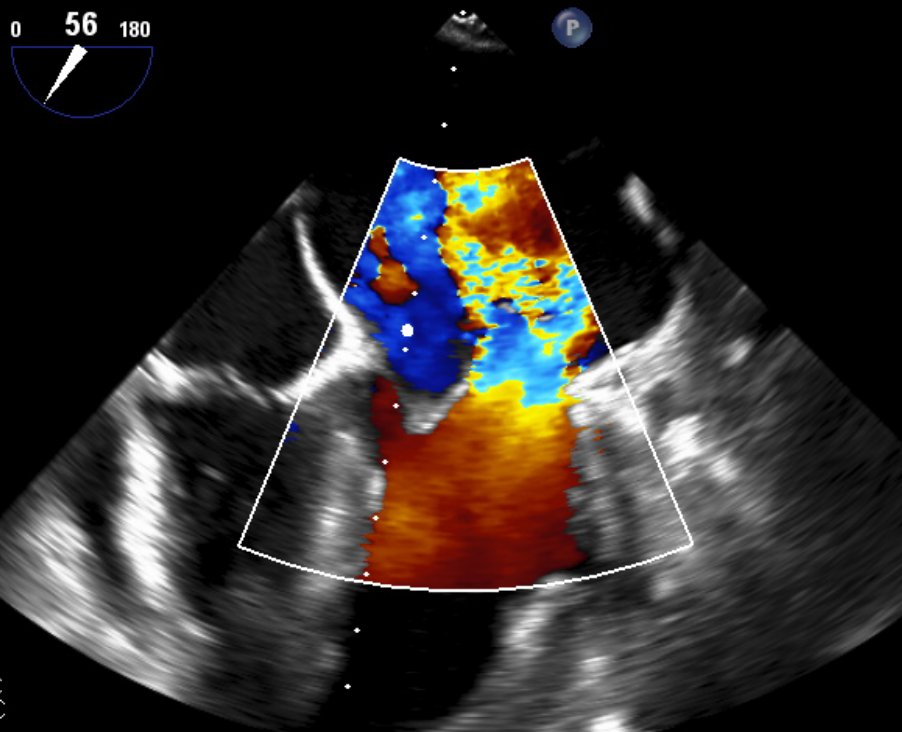
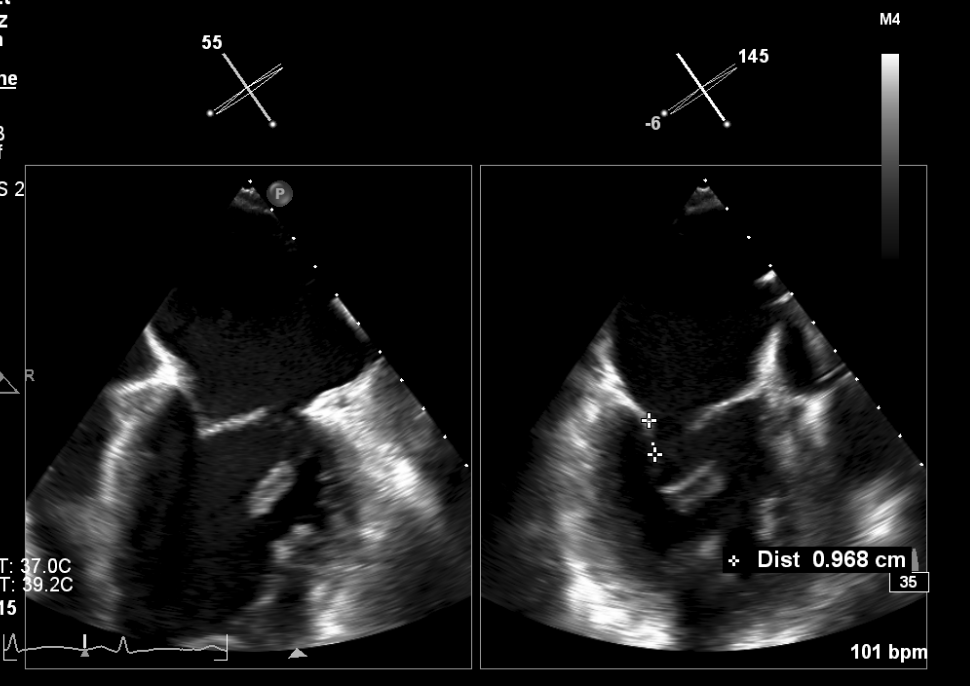
TOE: Torrential MR. There was flail anterior leaflet, constant movement of the papillary muscle with multiple subvalvular papillary chords. The posterior leaflet was restricted. The left atrial size was small (due to acute MR), which may prove challenging for transeptal puncture height.
Apologies, I was unable to include the video due to trouble with downloading video from the hospital system, will include in final presentation.
Relevant Catheterization Findings
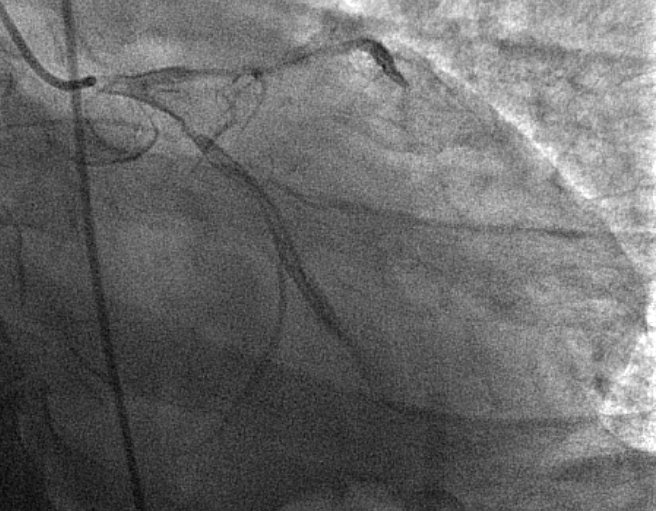
Angiogram was performed in referring centre and revealed LMCA guide-related dissection and LCx stent thrombosis. This was successfully treated with multiple stents to LMCA, LAD and LCx. Only single image was sent across to our system from the hospital.
This case was very recent, we apologise for incompleteness of images and videos.
This case was very recent, we apologise for incompleteness of images and videos.
Interventional Management
Procedural Step
This was a challenging anatomy as the posterior leaflet was restricted, constant papillary movement and multiple chord movement would impact on procedural success. The left atrium size was also small (due to acute MR), which may impact on puncture height. We elected for a PASCAL (Edwards Lifesciences, USA) device over Mitraclip (Abbott Cardiovascular, USA) as the PASCAL ACE system allows elongation of the device for minimal chord interaction, independent leaflet grasping and the ability to 'gain height' as the left atrium size was small.
We initially delivered the first ACE device at A2-P2 at 12-6 o'clock orientation to 'stabilise' the leaflets. This was challenging and took a long time, as the papillary muscle was constantly interacting with the device and reorientating the device. This caused a reduction in MR from torrential to severe, with the jet now mostly in the lateral commissures. A second device was delivered lateral to the first ACE device, at A1-P1 at 12-6 o'clock orientation. There was reduction in MR to moderate. The mean left atrial pressure reduced from 40 to 25 mmHg and there was loss of PV reversal. Mean mitral gradient was 6 mHg.
The patient had intropic support ceased the next day and VA-ECMO was decannulated. The patient's mitral surgery was delayed due to a ventilator associated pneumonia, causing poor oxygenation. Patient was alive on Day 5 (submission of this case report).
We initially delivered the first ACE device at A2-P2 at 12-6 o'clock orientation to 'stabilise' the leaflets. This was challenging and took a long time, as the papillary muscle was constantly interacting with the device and reorientating the device. This caused a reduction in MR from torrential to severe, with the jet now mostly in the lateral commissures. A second device was delivered lateral to the first ACE device, at A1-P1 at 12-6 o'clock orientation. There was reduction in MR to moderate. The mean left atrial pressure reduced from 40 to 25 mmHg and there was loss of PV reversal. Mean mitral gradient was 6 mHg.
The patient had intropic support ceased the next day and VA-ECMO was decannulated. The patient's mitral surgery was delayed due to a ventilator associated pneumonia, causing poor oxygenation. Patient was alive on Day 5 (submission of this case report).
Case Summary
Mitral edge-to-edge repair is feasible in acute MR in patients unsuitable for surgery or as a bridge to surgery. The aim is for reduction in severity of mitral regurgitation and improvement in mean LA pressure. The PASCAL ACE features of independent leaflet grasping, smaller device profile and small LA size may be useful in challenging anatomies