
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-021
Post Coronary Bypass Graft Intervention: Successful Percutaneous Coronary Intervention Through Left Internal Mammary Artery Conduit.
By Vipin Thomachan, Ali Shamsi, Gohar Jamil, Ahmed Siddiqui, Anwar Al Zaabi, Mohammed El-Harari, Sadek Mokahal, Andria Maria Badics, El Shafie Taha, Maha Al Ketbi, Khaled Shaheen, Soviachen Kurian, Sreekanth Saladi, Lizy George
Presenter
Vipin Thomachan
Authors
Vipin Thomachan1, Ali Shamsi1, Gohar Jamil1, Ahmed Siddiqui1, Anwar Al Zaabi1, Mohammed El-Harari1, Sadek Mokahal1, Andria Maria Badics1, El Shafie Taha1, Maha Al Ketbi1, Khaled Shaheen1, Soviachen Kurian2, Sreekanth Saladi1, Lizy George1
Affiliation
Tawam Hospital, United Arab Emirates1, Royal Hobart hospital, Australia2,
View Study Report
TCTAP C-021
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Post Coronary Bypass Graft Intervention: Successful Percutaneous Coronary Intervention Through Left Internal Mammary Artery Conduit.
Vipin Thomachan1, Ali Shamsi1, Gohar Jamil1, Ahmed Siddiqui1, Anwar Al Zaabi1, Mohammed El-Harari1, Sadek Mokahal1, Andria Maria Badics1, El Shafie Taha1, Maha Al Ketbi1, Khaled Shaheen1, Soviachen Kurian2, Sreekanth Saladi1, Lizy George1
Tawam Hospital, United Arab Emirates1, Royal Hobart hospital, Australia2,
Clinical Information
Patient initials or Identifier Number
HAU
Relevant Clinical History and Physical Exam
A 59year old male presented with non-ST elevation myocardial infarction (NSTEMI). He is known to have hypertension, dyslipidemia and coronary artery disease (CAD) with history of coronary artery bypass graft (CABG) surgery and percutaneous coronary intervention (PCI) about two years ago. Procedure was done elsewhere, and no details were available. History of worsening effort angina for the last few months. Clinically he was stable with BP142/92 mm Hg, HR 105bpm andspO2 99%.
Relevant Test Results Prior to Catheterization
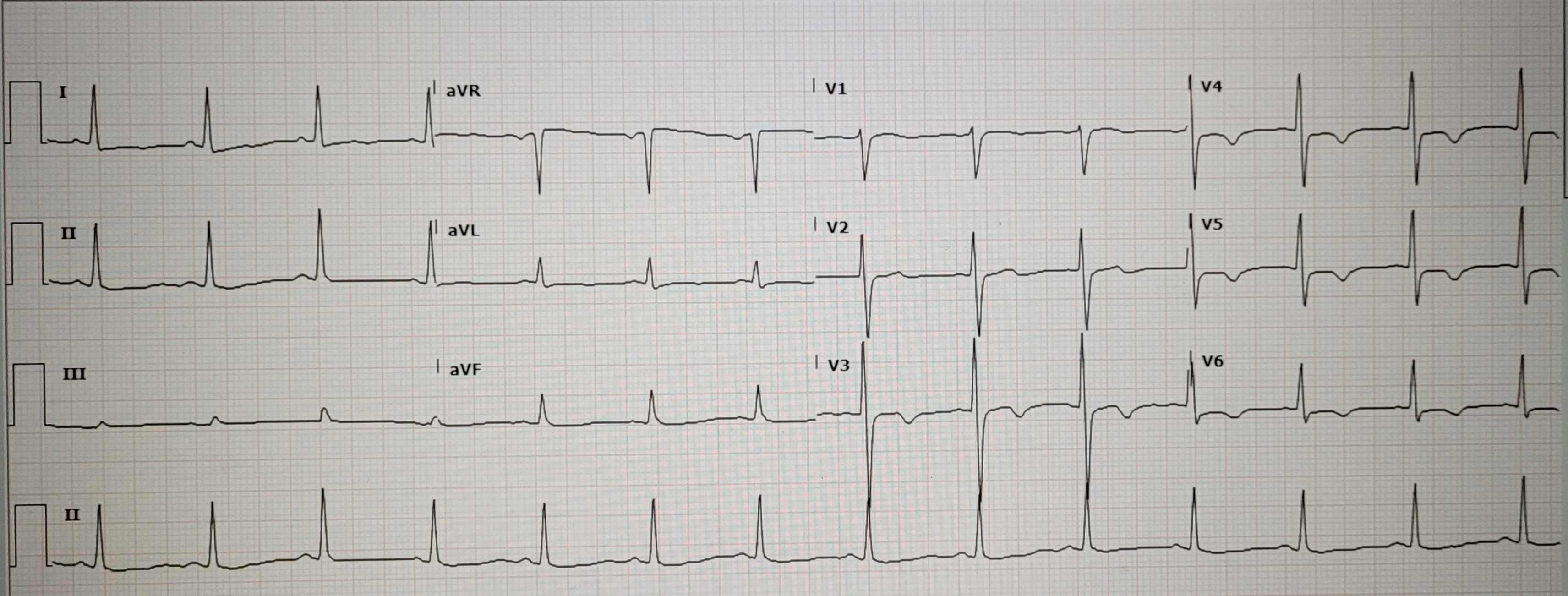
ECG showed sinus rhythm and T inversion in anterior leads. Initial cardiac Troponin was normal which peaked to a value of 248 ng/L subsequently. Renal function tests were normal. Echo showed normal EF (65%), no wall motion abnormalities, mild MR, TR and no PHTN. Patient was catheterized on next day after medical stabilization.
Relevant Catheterization Findings
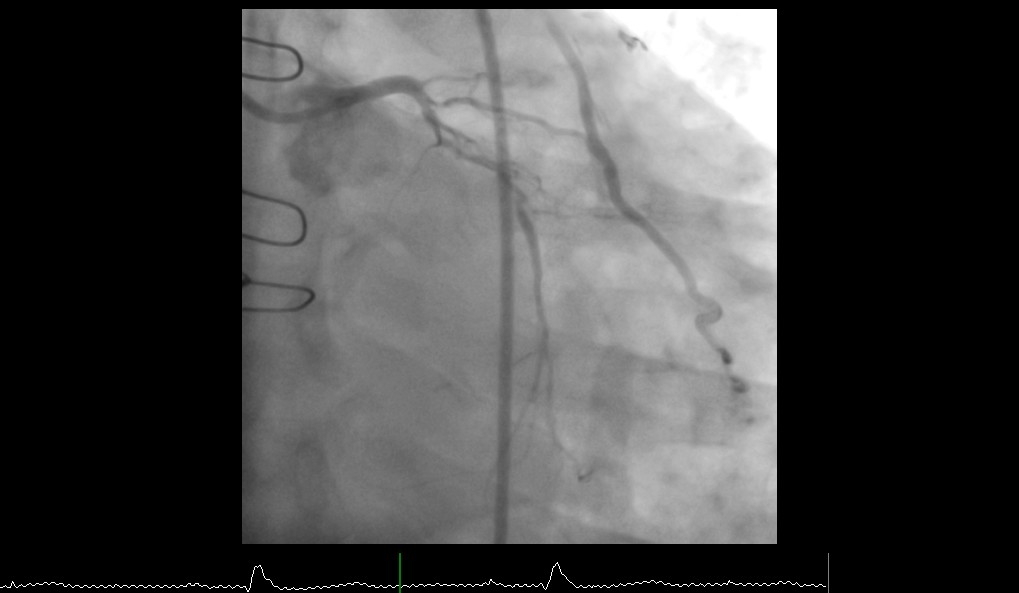
Coronary angiography was performed through right femoral arterial approach. Native vessel angiography revealed chronic total occlusion (CTO) from LAD ostium, severe proximal diffuse stenosis in an early OM with competitive flow from radial artery graft. Moderate to severe diffuse disease in proximal LCX. RCA had a patent stent in proximal segment, totally occluded small PDA and mild diffuse disease in PLV.
Interventional Management
Procedural Step
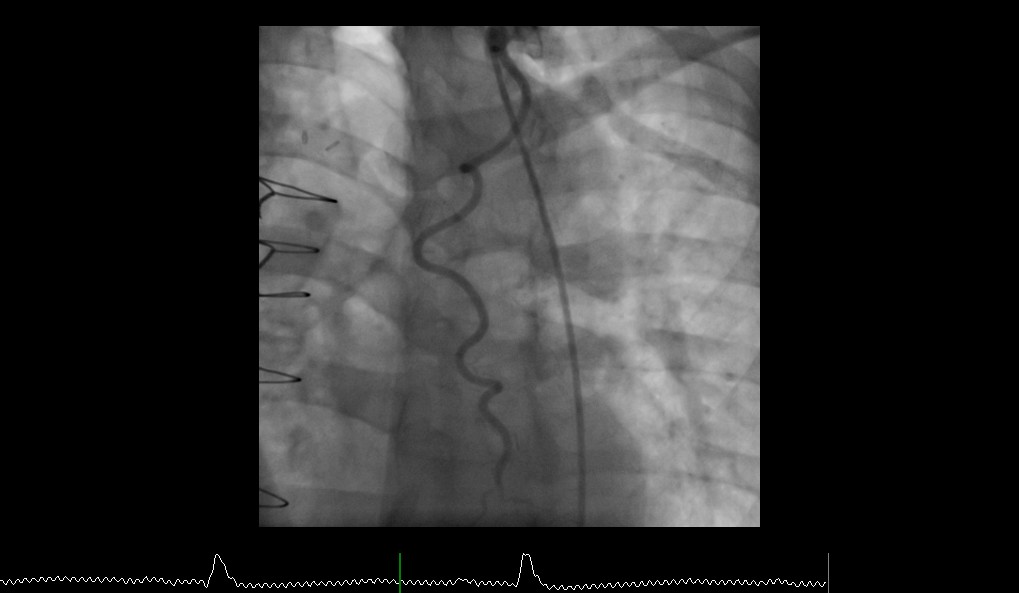
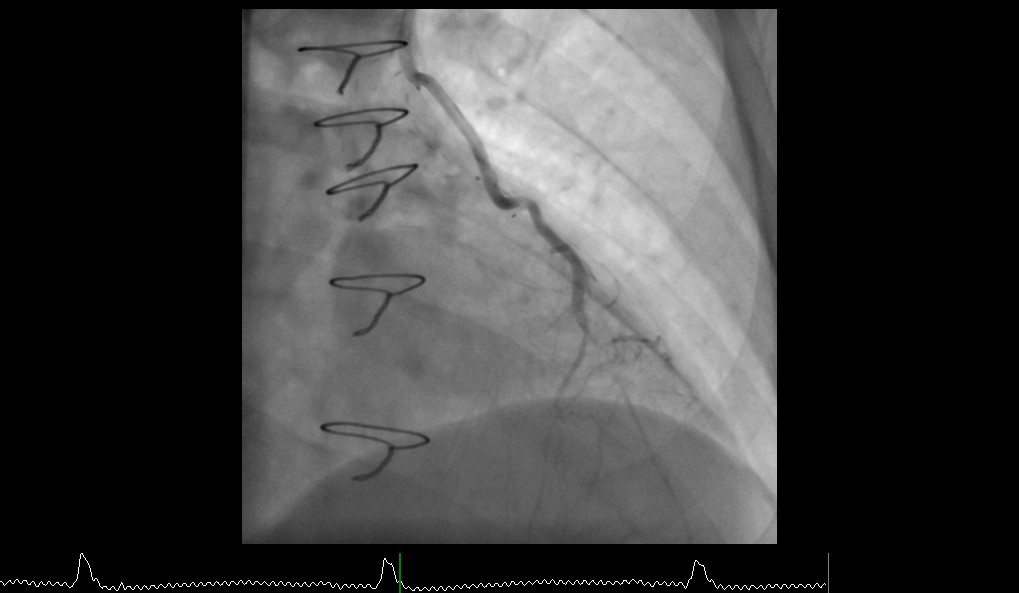
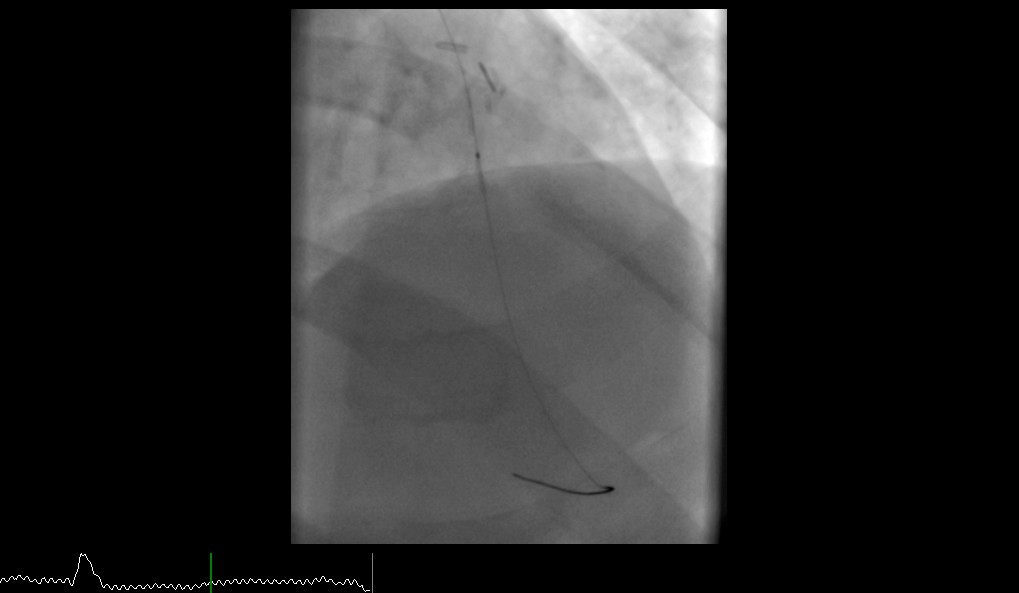
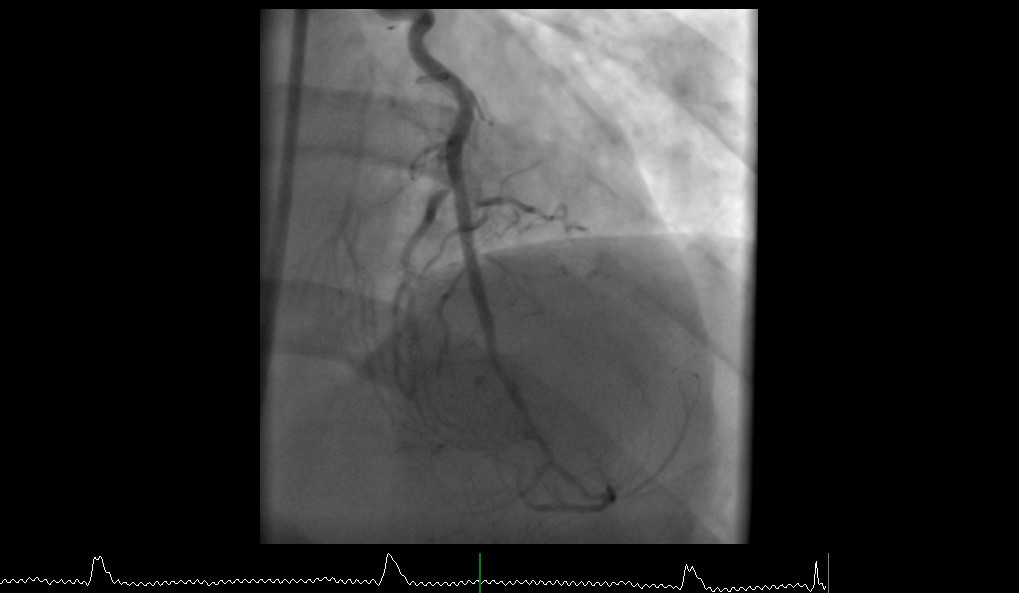
Graft angiography showed patent radial graft to principal OM. There was subtotal occlusion of left internal mammary artery (LIMA) graft to mid LAD anastomosis with severe lesions extending into native LAD resulting in faint antegrade flow. It was decided to carry out PCI of LIMA graft to LAD stenosis through LIMA graft conduit as native LAD had CTO.

Case Summary
Left internal mammary artery is the gold standard graft conduit with proven high patency rate for bypassing the LAD in coronary artery bypass graft surgery. It has been shown to be more durable than other arterial and vein grafts with a patency rate of >90% at 10years. Percutaneous coronary intervention through LIMA conduit is challenging especially through tortuous, redundant LIMA graft and it is associated with high risk of mortality. Here we demonstrate a case of successful coronary intervention of LIMA graft -LAD anastomotic site through LIMA graft conduit by a gentle and careful approach using appropriate hardware.