
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-069
LAD CTO Post CABG With Short Aneurysm
By Yen-Lien Chou
Presenter
Yen-Lien Chou
Authors
Yen-Lien Chou1
Affiliation
Tri-Service General Hospital, Taiwan1,
View Study Report
TCTAP C-069
CORONARY - Chronic Total Occlusion
LAD CTO Post CABG With Short Aneurysm
Yen-Lien Chou1
Tri-Service General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
1655423
Relevant Clinical History and Physical Exam
63-year-old man, non-smoker

Relevant Test Results Prior to Catheterization
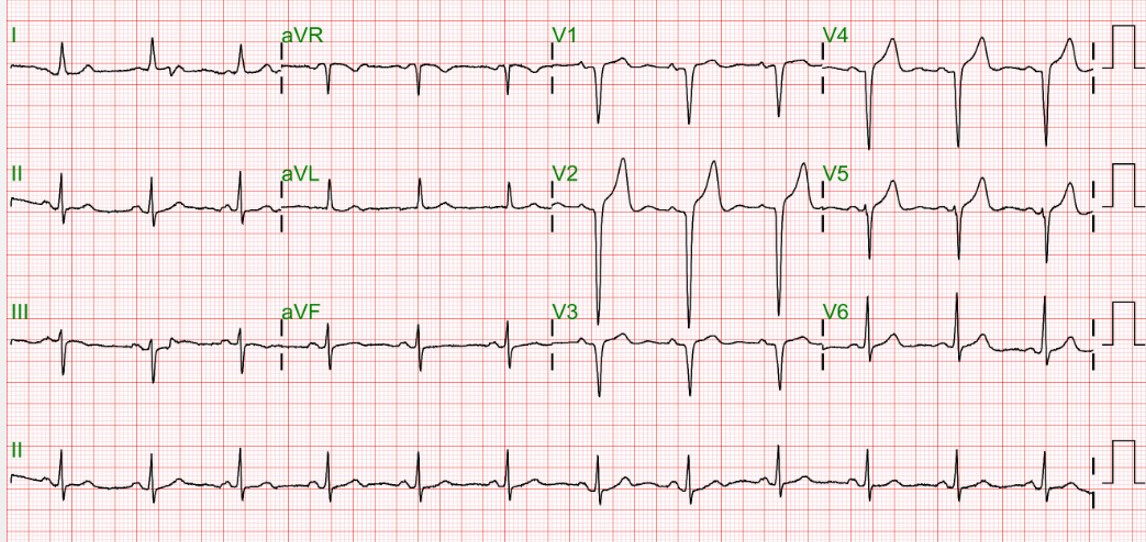
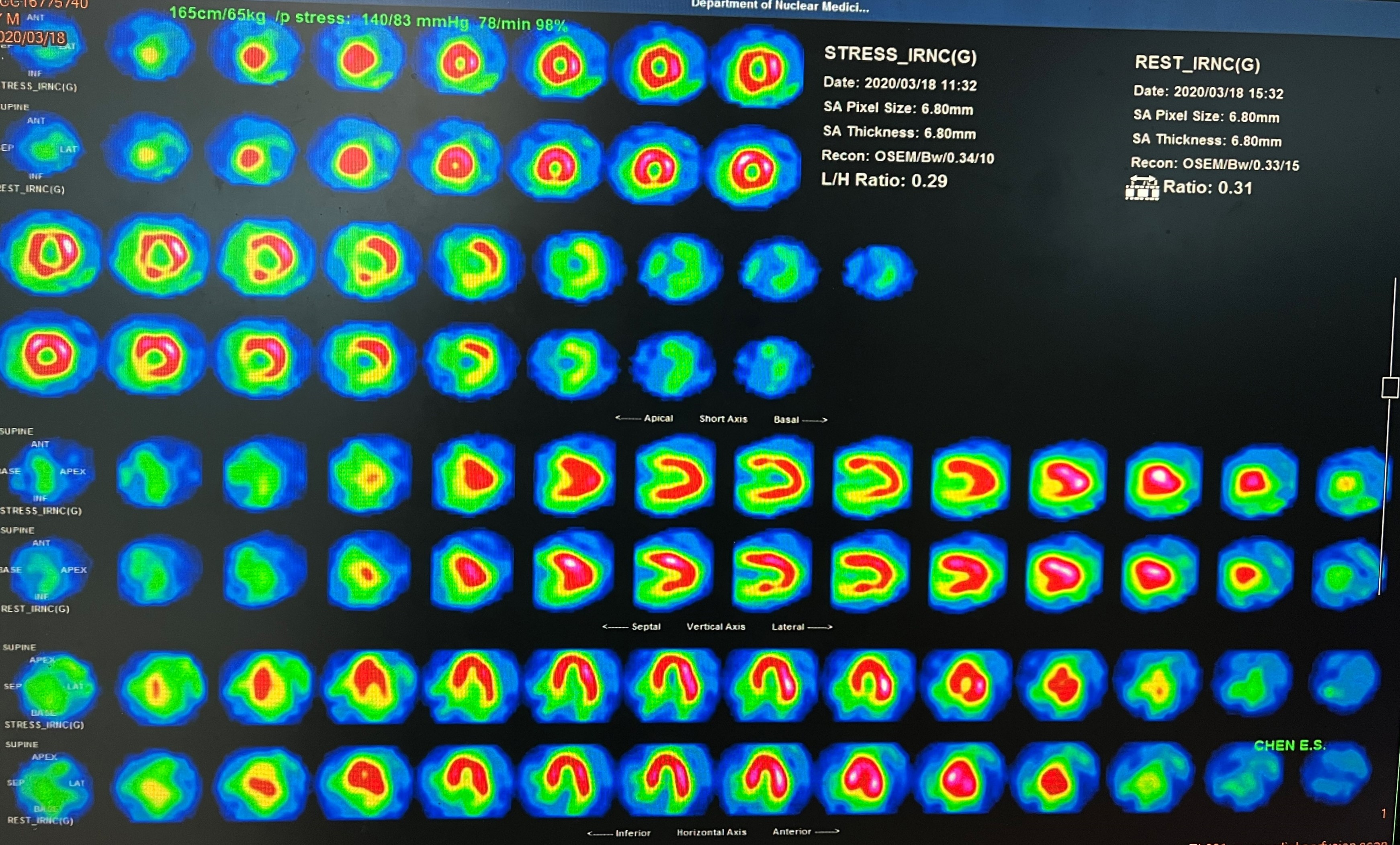
ECG showed sinus rhythm and QS pattern over V2-V4CXR revealed normal heart border and mild emphysematous change over bilateral lungEchocardiography showed preserved LVSF with EF: 70%, mild TR, Grade II diastolic dysfunction and PAP: 35mmHgTl-201 revealed ischemia over the anterior wall about 20-30%
Relevant Catheterization Findings
LM: patent, Medina (0,1,1)
 2.mp4
2.mp4
3.mp4
4.mp4
Interventional Management
Procedural Step
Antegrade approach from bilateral femoral artery
5.mp4
6.mp4
7.mp4
Case Summary
IVUS guidance for LAD ostium CTO is necessaryDouble lumen catheter is a good tool for LAD ostium CTO for increasing supportWhich is better ? LIMA Vs. LAD CTOVs. Do nothing