
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-123
Is Stronger Backup Always Better in Coronary Intervention?
By Ho Ling Tsoi
Presenter
Ho Ling Tsoi
Authors
Ho Ling Tsoi1
Affiliation
North District Hospital, Hong Kong, China1,
View Study Report
TCTAP C-123
CORONARY - Complications (Coronary)
Is Stronger Backup Always Better in Coronary Intervention?
Ho Ling Tsoi1
North District Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
LYK
Relevant Clinical History and Physical Exam
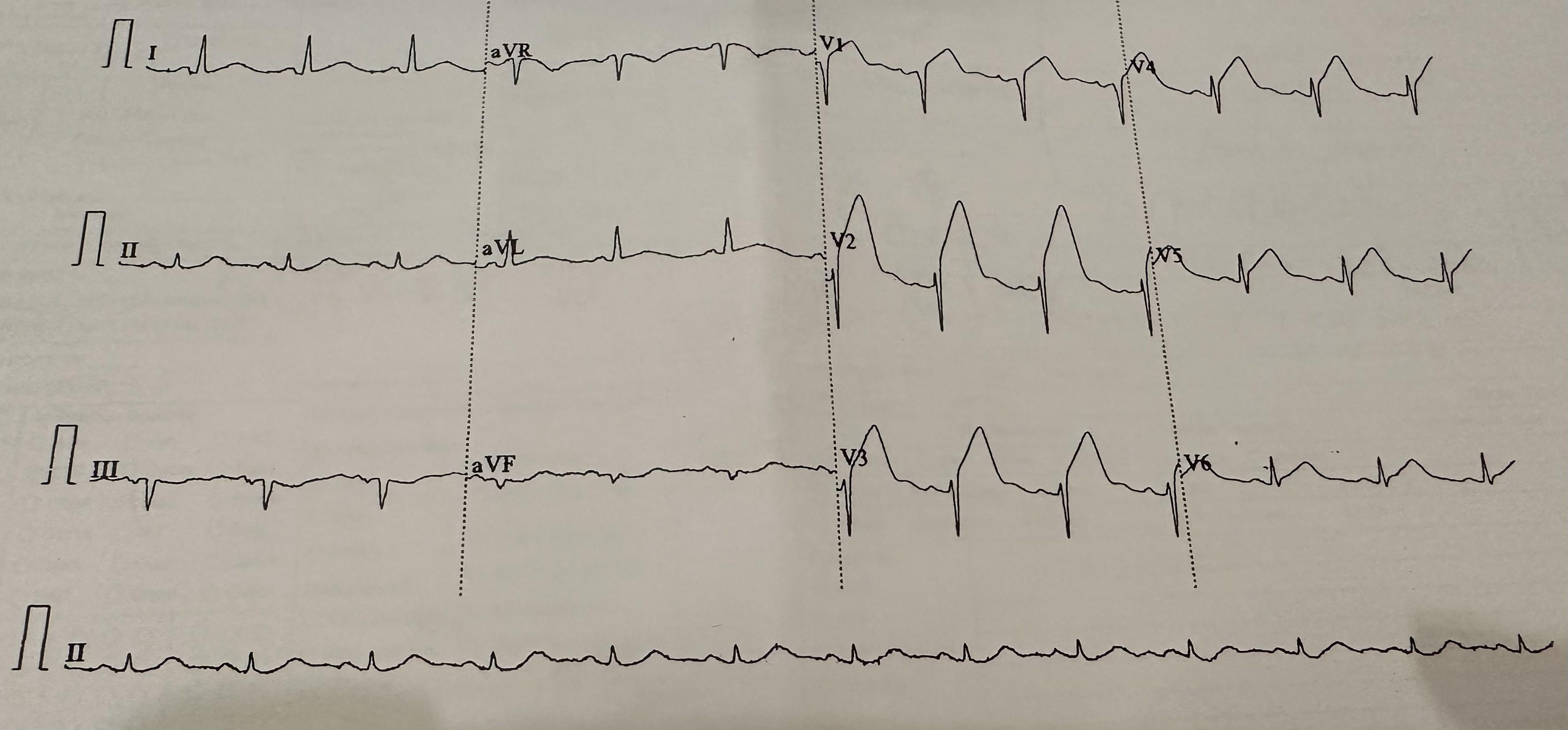
Ms LYK is a 67 years old lady with history of hyperlipidemia. She is a non-drinker and never smokes. Ms. LYK was first presented at AED with sudden onset central chest discomfort, associated with dyspnea and sweating. Physical examination showed normal heart sound without murmur and clear chest on auscultation. Initial ECG showed sinus rhythm 76bpm with ST-segment elevation over V1-6. Provisional diagnosis of anterior STEMI was made.
Relevant Test Results Prior to Catheterization
Echocardiogram showed LVEF 45% with concentric LVH. Akinesia over mid to apical anterior wall and anterior septum.
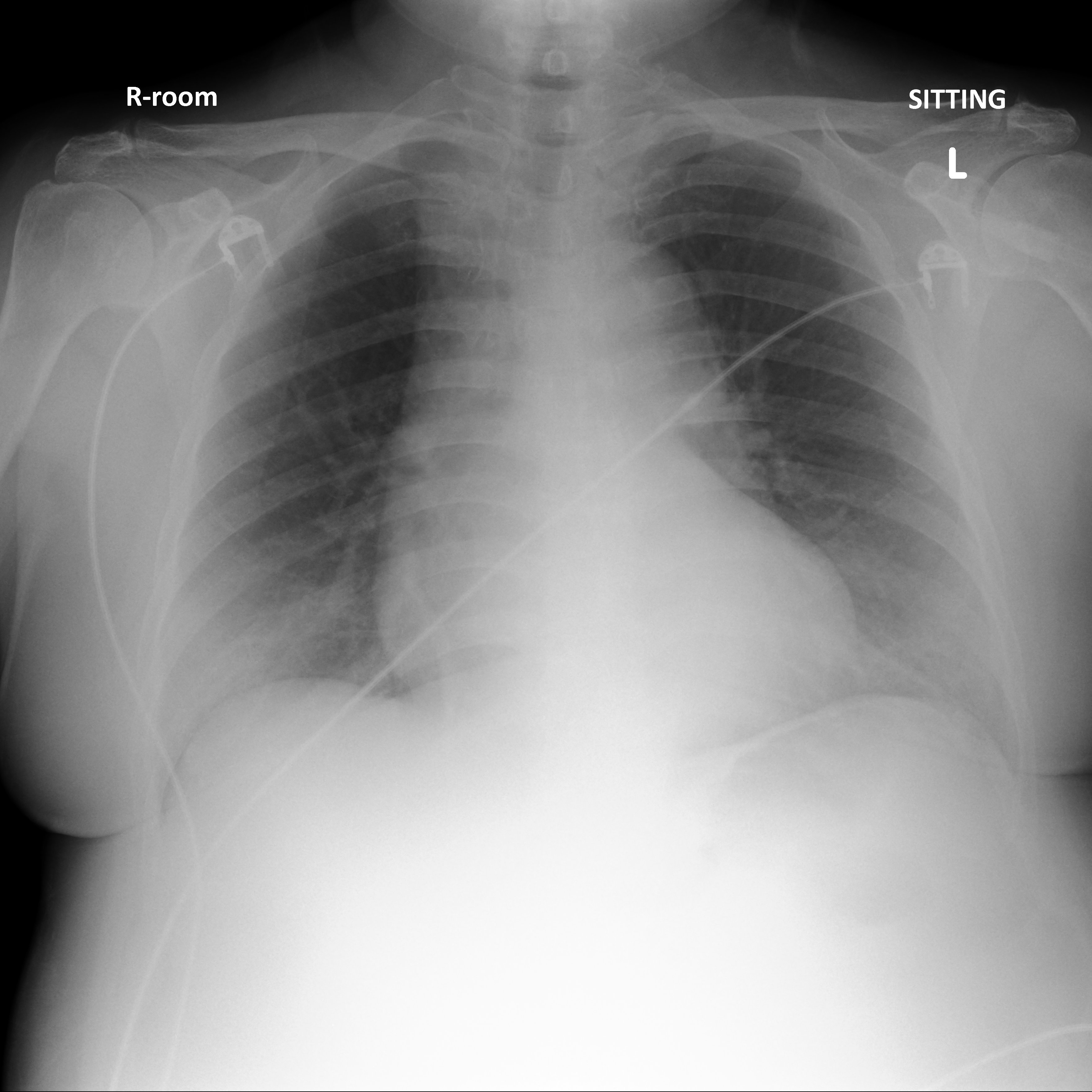
Chest X-ray showed no consolidation and no evidence of acute pulmonary edema
Baseline LDL level 5.6mmol/L
Intravenous thrombolytic therapy was given with successful reperfusion. Early PCI with stenting to mid-LAD was performed. Ms LYK was arranged stage PCI to LCx/OM subsequently
Relevant Catheterization Findings
Coronary angiogram (during STEMI) showed Left main 20%; mid-LAD 95% distal LAD 30%; OM branch 80%; RCA minor diseasePCI to mid-LAD (culprit lesion) with 3.0x18mm DES under IVUS guidance Stage PCI performed to LCx/OM. Initial angiogram showed no significant ISR over LAD stent.


Interventional Management
Procedural Step
Right radial approach. 6Fr JL4 guiding catheter. Runthrough wire to OM. Predilated OM with NC Scoreflex 2.25x10mm. Stenting to pLCx/OM with 2.5 x 24mm (Synergy) DES.Attempted post dilatation to stent but unable to pass NC balloon (2.25x10mm) with extra wire support to OM. Switched to EBU 3.5 6Fr guiding catheter and wiring to OM with same Runthrough wire. Finally able to post dilate stent with NC 2.25 x 10mm then NC 3.0 x 12mm with guiding extension catheter support. Post dilatation angiogram showed contrast stained over LM and aortic root. LAD immediately wired with another Runthrough wire. IVUS to both LAD-LM and LCx-LM done, showing intramural hematoma from ostial LM to pLCx and mLAD. Attempted to stent from ostial LM to LCx but failed to advance stent. Ms LYK developed chest discomfort, hypotension and bradycardia. She was given atropine injection and dopamine infusion for support. Later decided to pass stent from ostial LM to LAD with 4.0 x24mm (Synergy) DES. IVUS showed good stent apposition. LCx rewired with Sion wire and ostial LCx stent cell opened with 2.5x10mm balloon. Minimal contrast stain over aortic root / LM at final angiogram. Repeated bedside echocardiogram showed no pericardial effusion. CT aortogram (post PCI) showed acute IMH along aortic root, ascending aorta, towards the proximal aortic arch. No active extravasation and no hemopericardium was seen. Consulted CTS team and suggested close obersvation with blood pressure control.



Case Summary
Ms LYK had stable hemodynamics and remained asymptoamtic. Repeated CT aortogram (day 2 post PCI) showed interval improvement of intramural hematoma with 0.5cm thickness. Ms LYK was later discharged home after one week of close monitoring. Reangiogram arranged one month later showed no significant ISR to both LM/LAD and LCx/OM stent. No residual IMH.
Stronger backup force with guiding catheter plus guiding extension catheter support will facilitate better delivery of balloon or stent to our target. However, we should also consider the drawback of this strategy might lead to detrimental result. Stronger is not always better in the setting of tortious LCx lesion
Stronger backup force with guiding catheter plus guiding extension catheter support will facilitate better delivery of balloon or stent to our target. However, we should also consider the drawback of this strategy might lead to detrimental result. Stronger is not always better in the setting of tortious LCx lesion