
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-207
Paravalvar Device Closure in a 11YR Child With Re-Re Do MVR
By Sumanta Shekhar Padhi
Presenter
Sumanta Shekhar Padhi
Authors
Sumanta Shekhar Padhi1
Affiliation
Raipur-MMI Narayana Superspeciality Hospital, India1,
View Study Report
TCTAP C-207
STRUCTURAL HEART DISEASE - Valvular Intervention: Mitral or Tricuspid
Paravalvar Device Closure in a 11YR Child With Re-Re Do MVR
Sumanta Shekhar Padhi1
Raipur-MMI Narayana Superspeciality Hospital, India1,
Clinical Information
Patient initials or Identifier Number
HB
Relevant Clinical History and Physical Exam
11y/F.PAVCD repaired 9.17(Dacron patch closure of OP ASD & cleft AML repair ).F.U at 1 ½ yr -Sev MR & PAH, Good LV , Fc IV- despite maximal medications. Planned for MVR .Re-Do MVR (4.12.19) done by thoracotomy . A 25mm St Jude mechanical prosthesis was used with pledgeted sutures. A small PVL at 3 ‘O’ position after surgery. Extubated on 1st POD. On 5th POD- LVF- needed NIV. ECHO: Sev MR through 3 PVLs, Mod PAH.Refractory CHF despite OMT. Planned for PVL deviceclosure-17th POD.
Relevant Test Results Prior to Catheterization
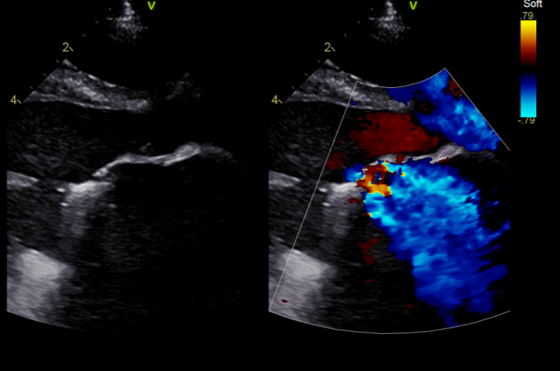
TTE followed by TEE showed 3 PVLs : 2mm, 3mm and 5mm size at the aortomotral curtain. The prothetic valve function and LV was normal.
Relevant Catheterization Findings
PA pr- 40/26 mmHg
Interventional Management
Procedural Step
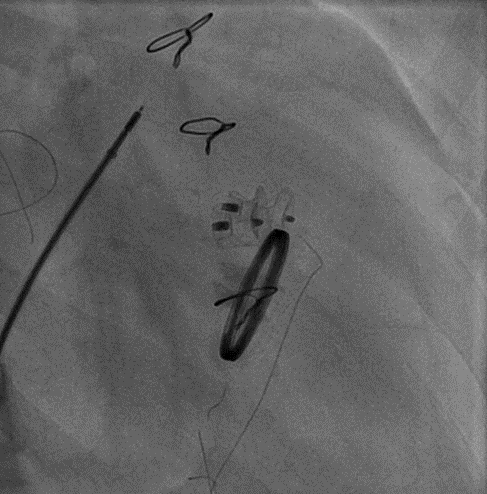
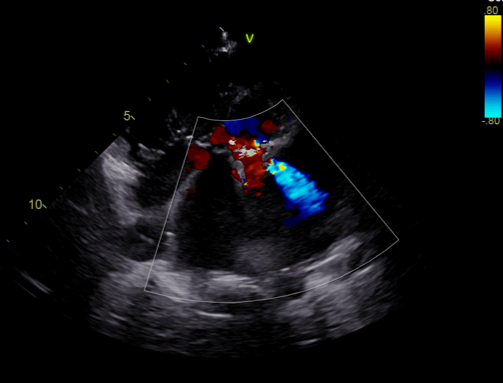
Rt FV was stenosed due to previous cannulation. Neededdilatation. For The curve in the Brokenbrough needle needed a larger curve for the septal puncture. The septal puncturewas difficult due to Dacracon patch. One of the PVL was crossed withRetrogradely with Turmo exchange wire, snared in LA, AV loop was made and througha 7F sheath a 10-8 ADO I device was deployed from the venous end. There wassignificant residual leak. The lesion was again crossed and AV loop made. Thistime 5F Sheath was used as 7F sheath could not be crossed. A 8-6 ADO I wasdeployed and the leak closed. Post procedure only tiny leak was left. Theresult was accepted
Case Summary
Post procedure the child could be extubated with in 12 hrand could be discharge after 5 days after optimization of OAC.