
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-148
A Lucky Bail Out in a Case of Fractured Tip of Diagnostic Catheter
By Khairul Shafiq Ibrahim, Loi Hoang, Kan Latthanngam, Sorracha Rookkapan
Presenter
Khairul Shafiq Ibrahim
Authors
Khairul Shafiq Ibrahim1, Loi Hoang2, Kan Latthanngam3, Sorracha Rookkapan3
Affiliation
Universiti Teknologi MARA (UiTM), Malaysia1, Hanoi Heart Hospital, Vietnam2, Prince of Songkla University, Thailand3,
View Study Report
TCTAP C-148
ENDOVASCULAR - Complications (Endovascular)
A Lucky Bail Out in a Case of Fractured Tip of Diagnostic Catheter
Khairul Shafiq Ibrahim1, Loi Hoang2, Kan Latthanngam3, Sorracha Rookkapan3
Universiti Teknologi MARA (UiTM), Malaysia1, Hanoi Heart Hospital, Vietnam2, Prince of Songkla University, Thailand3,
Clinical Information
Patient initials or Identifier Number
JB
Relevant Clinical History and Physical Exam
Mr JB is a 64 year-old man smoker with history of aortoiliac occlusive disease and right common iliac artery occlusion which was treated with covered endovascular reconstruction of aortic bifurcation in 2019. He has been complaining of intermittent claudication over his right leg for the past one year and its progressively worsening. On examination, both feet were warm with no ulcers nor discolouration. All peripheral pulses were palpable but ankle brachial index of right leg was 0.74.
Relevant Test Results Prior to Catheterization
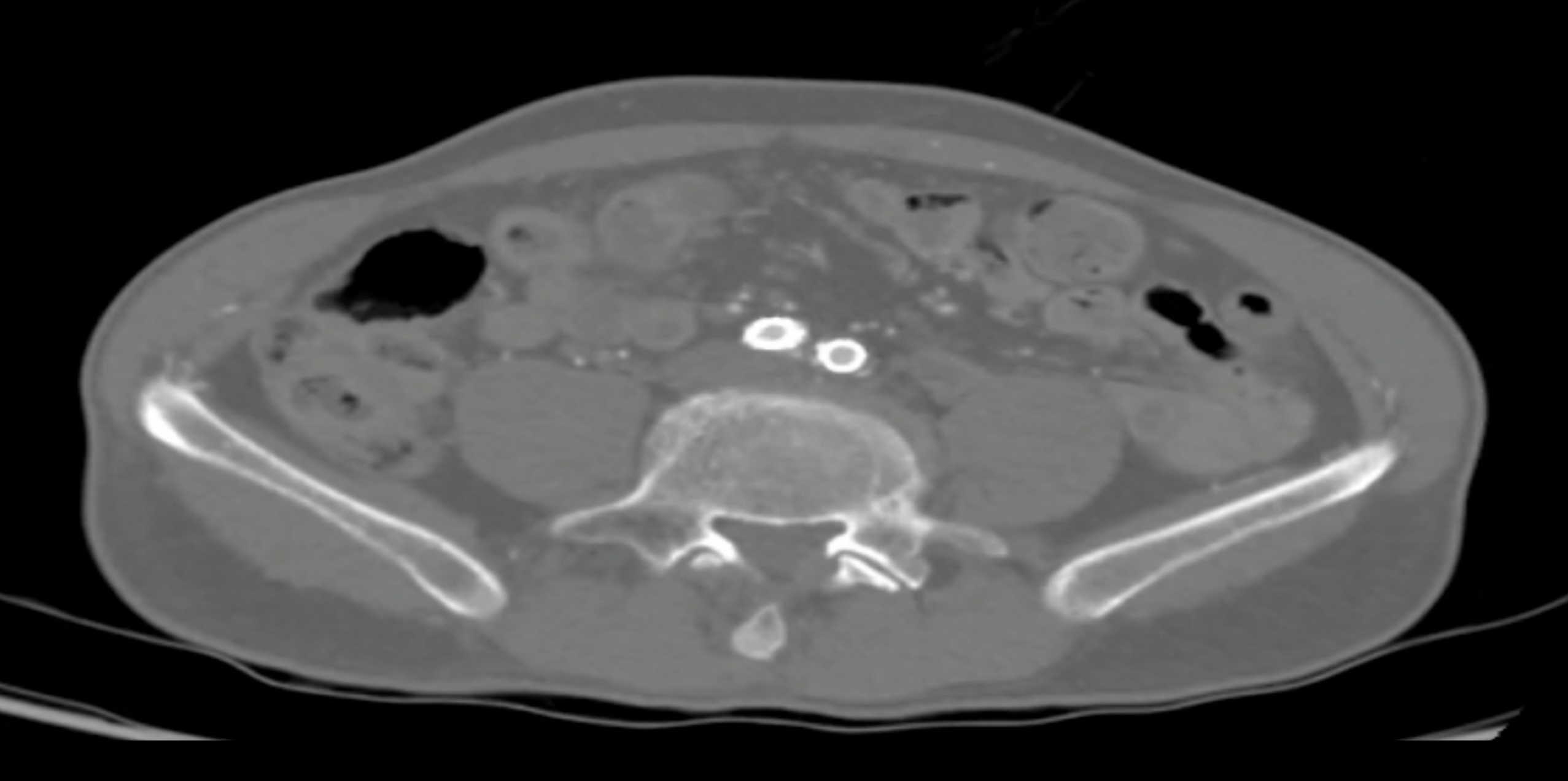
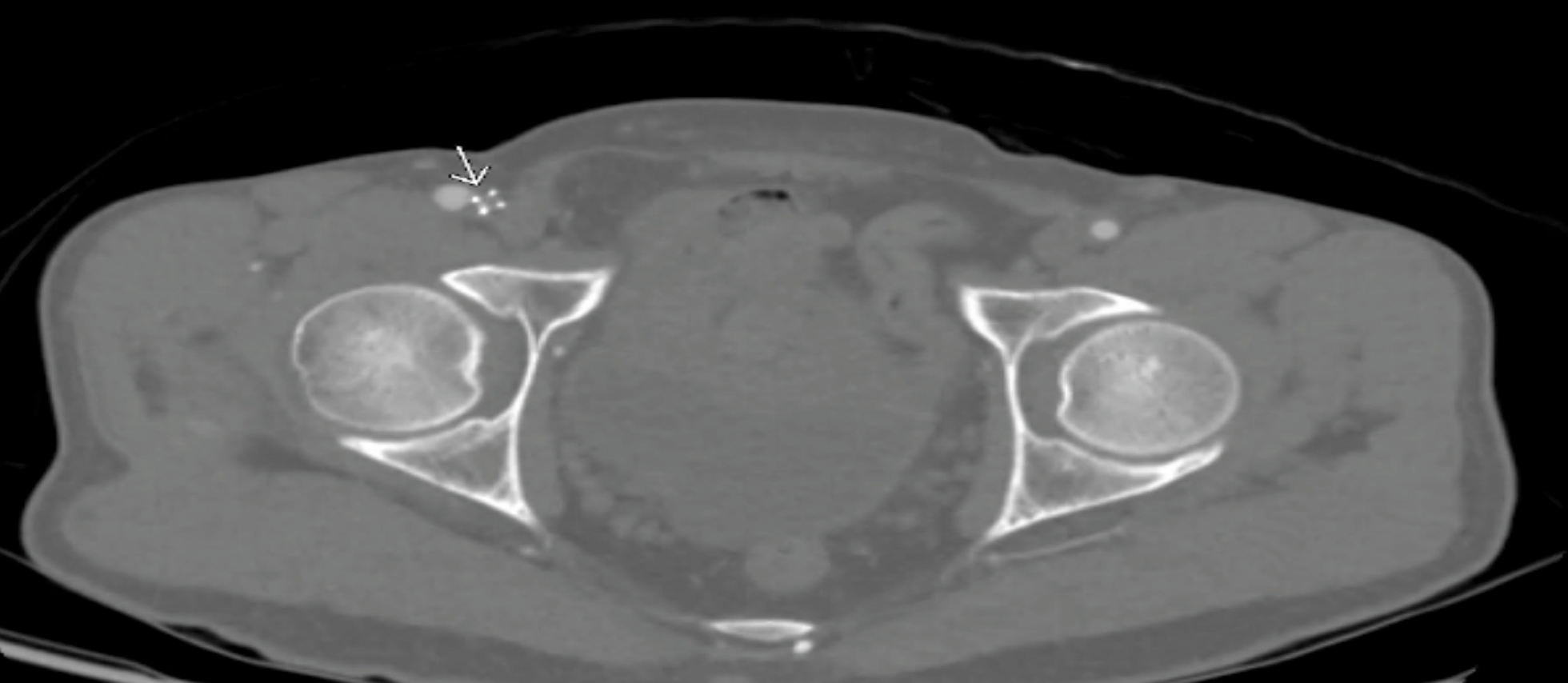
His haemoglobin was 13.9 g/dl, platelet of 190,000/microlitre and GFR of 87mL/min/1.73m2Contrast-enhanced computed tomography showed moderate in-stent restenosis at the right common iliac artery (CIA) and severe stenosis proximal to proximal edge of stent at the right superficial femoral artery (SFA) (Figure A and B).
Relevant Catheterization Findings
Angiography performed via left brachial artery with pigtail catheter showed moderate in-stent restenosis at the overlapped segment in right CIA. Severe stenosis was demonstrated at the proximal edge of the SFA stent (Figure C).

Interventional Management
Procedural Step
6Fr Durasheath 90cm was inserted via the left brachial artery. A 5Fr 125cm angulated microcatheter over a stiff 0.035 wire was used to assist wiring into SFA. Unfortunately, the tip of the microcatheter was fractured when the distal part of it was made into a loop and pulled back from the profunda artery into CFA. The 0.035 wire was accidentally pulled back, leaving the fractured tip hanging in the right CFA (Figure D). Multiple attempts were made to snare the tip through the brachial approach but unsuccessful. Hence we decided to attempt retrograde wiring into the ruptured tip via the popliteal artery. If unsuccessful, the plan was to put a stent across the ruptured tip to prevent its migration distally.
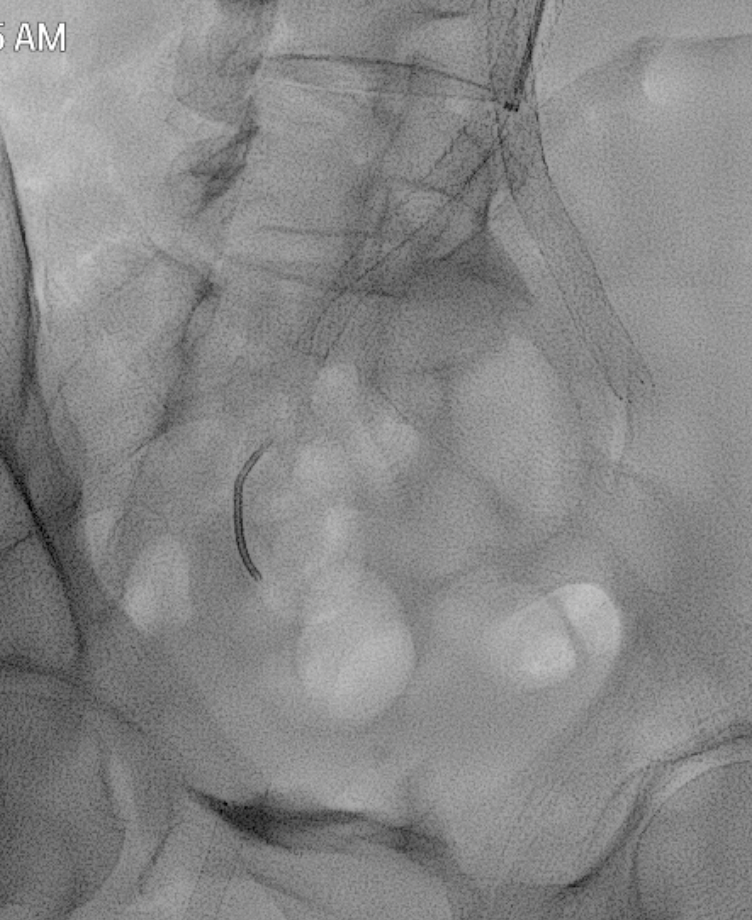
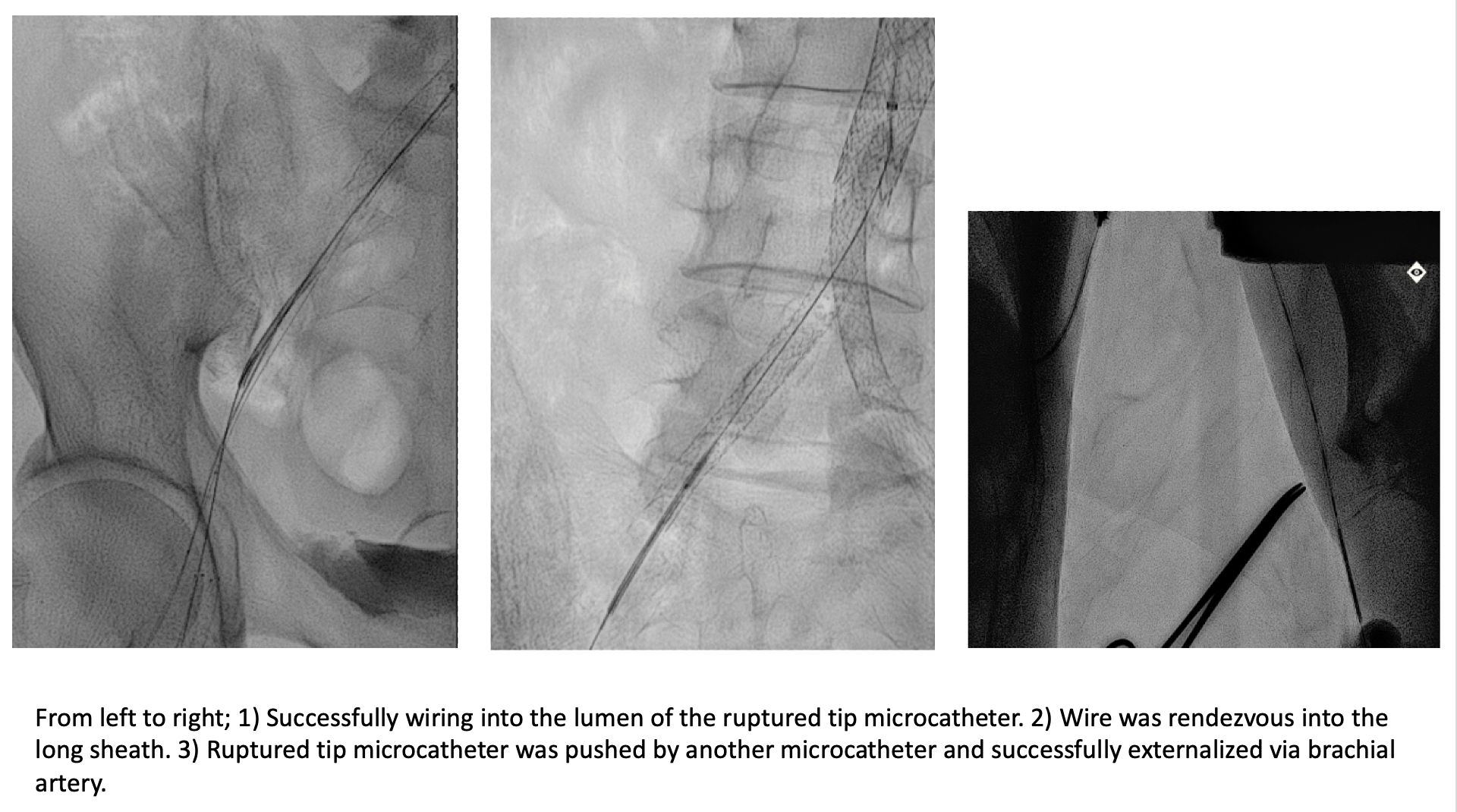
 Figure E removing the fractured tip.png
Figure E removing the fractured tip.png
Popliteal access was secured and 0.018 wire with microcatheter was successfully advanced across the lesion at the proximal SFA. Luckily the wire went through the lumen of fractured microcatheter and successfully rendezvous into the long sheath and externalized at the left brachial artery (Figure E). A microcatheter was used to push the ruptured tip out of the long sheath.
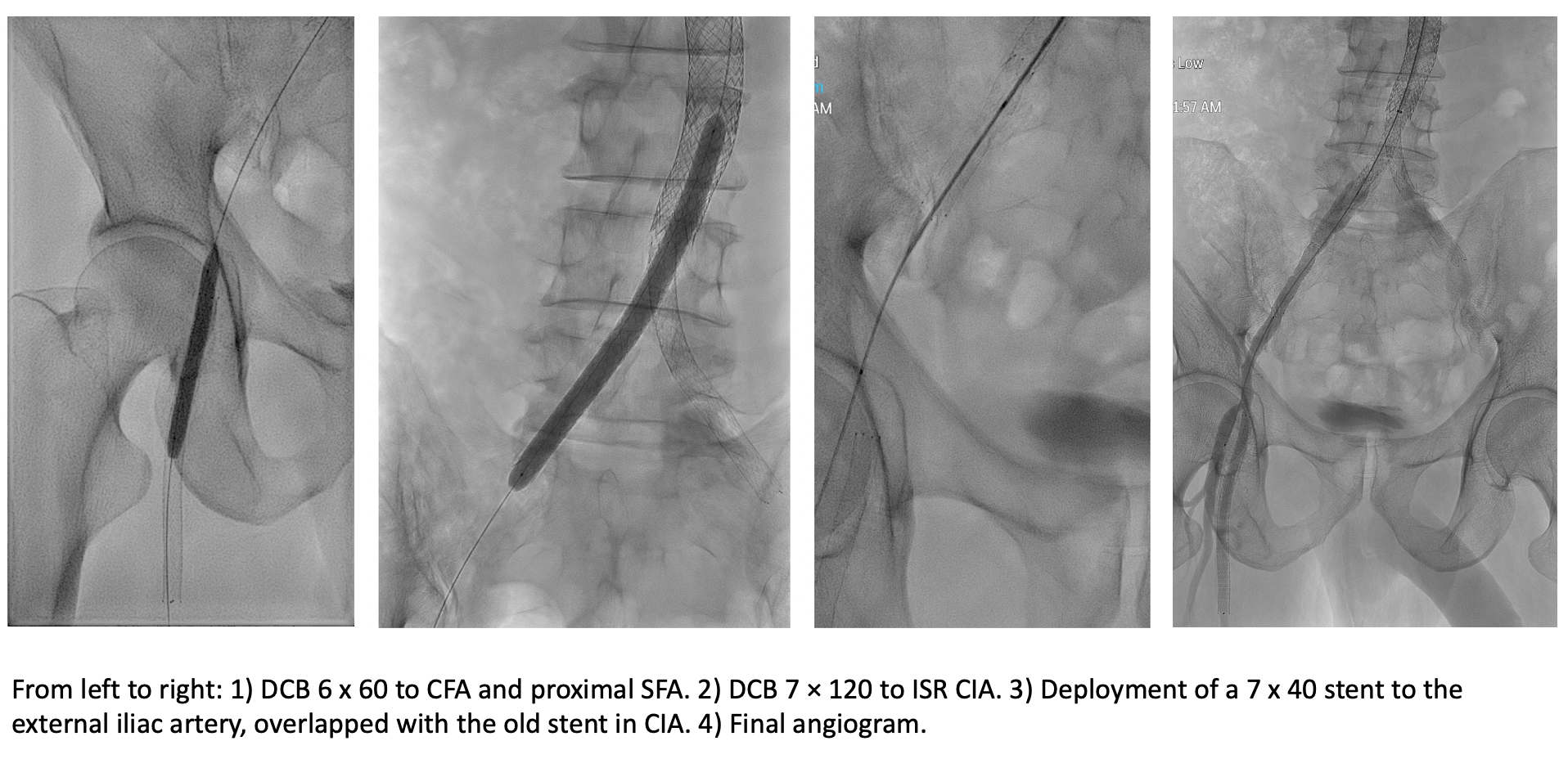
The procedure was continued with dilatation of the ostial SFA and the common iliac artery (CIA) with a 6.0 x 60mm balloon. Drug coating balloon 6 x 60mm and 7 x 120mm was applied to ostial SFA and CIA respectively. Another 7 x 40mm self-expanding stent was deployed at right external iliac artery, overlapped with the old stent (Figure F). Final angiography showed no dissection or recoil and good flow distally.
Case Summary
Delicate handling of microcatheter should be practised at all times to prevent this complication. In this case, we successfully retrieved the fractured tip of the microcatheter by rewiring into its lumen and pushing it out through the left brachial artery sheath using a support catheter. In case of unsuccessful wiring, the option to stent across the fractured segment against the vessel wall should be considered. This will prevent distal migration of the fractured tip which can cause occlusion of the distal vessel.