
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-024
Shocking the Uncrackable Calcium
By Wei Juan Lim, Mugilan Sundarajoo, Kumara Gurupparan Ganesan
Presenter
Wei Juan Lim
Authors
Wei Juan Lim1, Mugilan Sundarajoo2, Kumara Gurupparan Ganesan1
Affiliation
National Heart Institute, Malaysia1, National Heart Institute Ijn, Malaysia2,
View Study Report
TCTAP C-024
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Shocking the Uncrackable Calcium
Wei Juan Lim1, Mugilan Sundarajoo2, Kumara Gurupparan Ganesan1
National Heart Institute, Malaysia1, National Heart Institute Ijn, Malaysia2,
Clinical Information
Patient initials or Identifier Number
RDN
Relevant Clinical History and Physical Exam
64 years old gentleman with underlying hypertension and dyslipidemia presented to our center for typical angina for 1-dayduration. It was pressing in nature with radiation to arm associated with shortness of breath. Physical examination was unremarkable with blood pressure 120/70mmHg and pulse rate 76bpm.



Relevant Test Results Prior to Catheterization
Electrocardiogram (ECG) showed T inversion anterior leads with raised Troponin T of 218pg/ml. A diagnosis of non-ST elevation myocardial infarction (NSTEMI) was made. Echocardiogram showed left ventricular function (LVEF) of 55% with normal valves.
Relevant Catheterization Findings
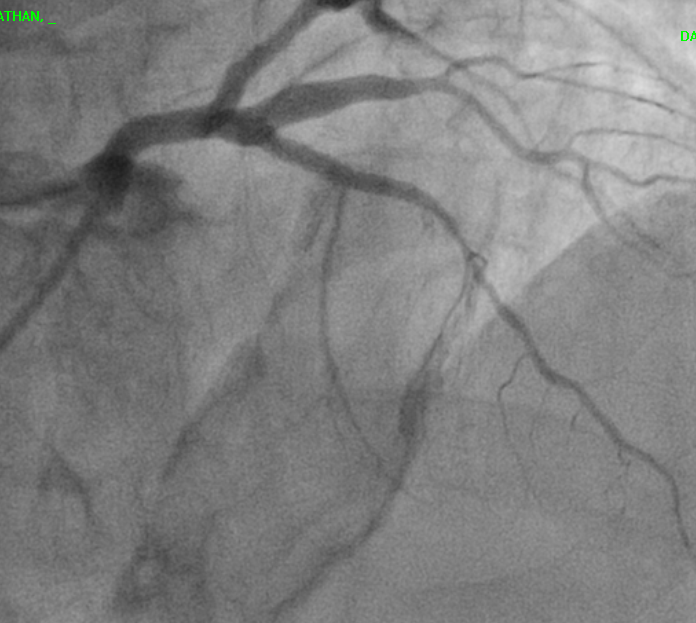
Coronary angiogram showed significant stenosisof ostial to proximal left anterior descending (LAD) artery with calcified plaque.The other coronary arteries were huge with no significant stenosis.
Interventional Management
Procedural Step
This patient came in with typical angina with raised troponin T. Initial coronary angiogram showed huge coronary arteries, misleading the huge diagonal as LAD on caudal and spider view. On Cranial view we can notice the LAD is actually diffusely disease with significant calcium load. The LAD vessel size is significantly smaller than the huge diagonal as well.
We have decided to treat the LAD lesion in view of NSTEMI with chest pain.
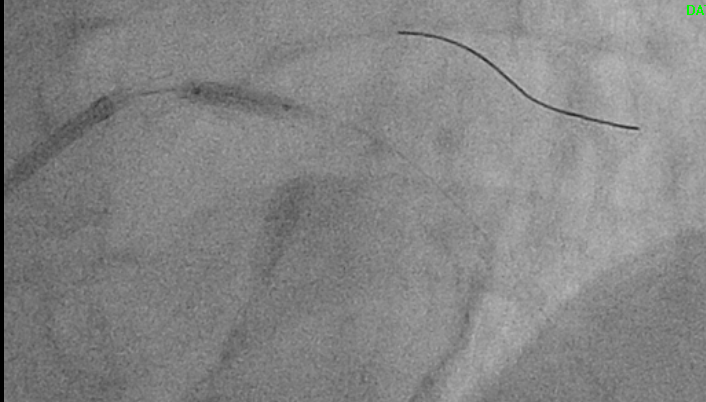
Sion blue wired down to LAD with runthrough floppy protecting the big diagonal branch. Initial plan was to use Scoreflex NC (Non-compliance) 2.0 x 15mm balloon to open up the calcified plaque but lesion was tight and could not crack the lesion. We have upsized the scoring balloon to Scoreflex NC 2.5x15mm but to no avail. Decision was made to use intravascular lithotripsy (IVL) to break the calcified plaque. IVL balloon size 3.0x12mm was chosen and with 30 pulses of shockwave, we were able to open up the tight calcified lesion. Calcified lesion was then further prepared with Scoreflex NC 3.0x15mm balloon.
Lesion was stented with Xience Sierra 3.0 x28mm and then post-dilated with NC balloon 3.5 x 15mm with good result. Post-stenting angiogram showed TIMI 3 flow with no dissection.

We have decided to treat the LAD lesion in view of NSTEMI with chest pain.
Sion blue wired down to LAD with runthrough floppy protecting the big diagonal branch. Initial plan was to use Scoreflex NC (Non-compliance) 2.0 x 15mm balloon to open up the calcified plaque but lesion was tight and could not crack the lesion. We have upsized the scoring balloon to Scoreflex NC 2.5x15mm but to no avail. Decision was made to use intravascular lithotripsy (IVL) to break the calcified plaque. IVL balloon size 3.0x12mm was chosen and with 30 pulses of shockwave, we were able to open up the tight calcified lesion. Calcified lesion was then further prepared with Scoreflex NC 3.0x15mm balloon.
Lesion was stented with Xience Sierra 3.0 x28mm and then post-dilated with NC balloon 3.5 x 15mm with good result. Post-stenting angiogram showed TIMI 3 flow with no dissection.
Case Summary
Initial pre-dilatation with scoring balloon was not successful and a decision to change to IVL was a good choice as we can see the calcified lesion was cracked open after 30 pulses of shockwave. The LAD vessel was significantly bigger after stenting with post-dilatation as compared to the initial image. This case illustrated the importance to treat the prognostication LAD vessel with appropriate device for a calcified lesion such as IVL. We should not pre-judge any lesion based on the initial image alone.