
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-022
Association of Stress Hyperglycemia With Long-Term Mortality After Acute Myocardial Infarction in Patients With or Without Diabetes.
By Guyu Zeng, Deshan Yuan, Jinqing Yuan
Presenter
Guyu Zeng
Authors
Guyu Zeng1, Deshan Yuan1, Jinqing Yuan1
Affiliation
Fuwai Hospital, China1
View Study Report
TCTAP A-022
Acute Coronary Syndromes (STEMI, NSTE-ACS)
Association of Stress Hyperglycemia With Long-Term Mortality After Acute Myocardial Infarction in Patients With or Without Diabetes.
Guyu Zeng1, Deshan Yuan1, Jinqing Yuan1
Fuwai Hospital, China1
Background
Admission glucose level and stress hyperglycemia ratio (SHR) are both common indicator of stress hyperglycemia. However, it is controversial whether SHR has better prognostic value for long-term mortality than admission glucose in patients with acute myocardial infarction (AMI).
Methods
A total of 5,832 AMI patients from a large nationwide prospective cohort enrolled between January 2015 and July 2019 were included [median follow-up period: 2.1 years (interquartile range: 2.0-2.1 years)]. SHR was calculated by the following formula: SHR=admission glucose (mmol/L)/[1.59×HbA1c (%)-2.59]. The primary endpoint was all-cause mortality during follow-up.
Results
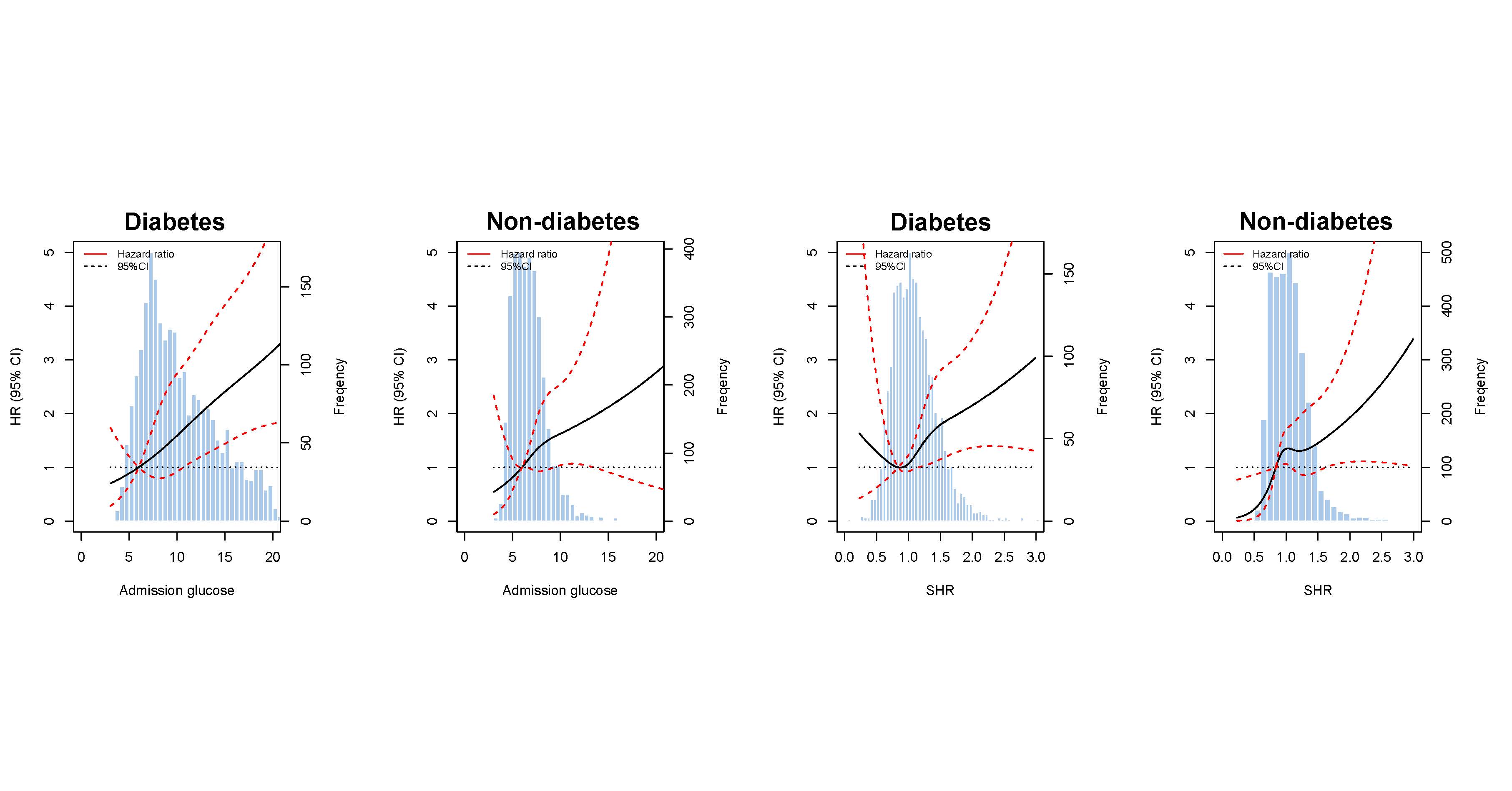
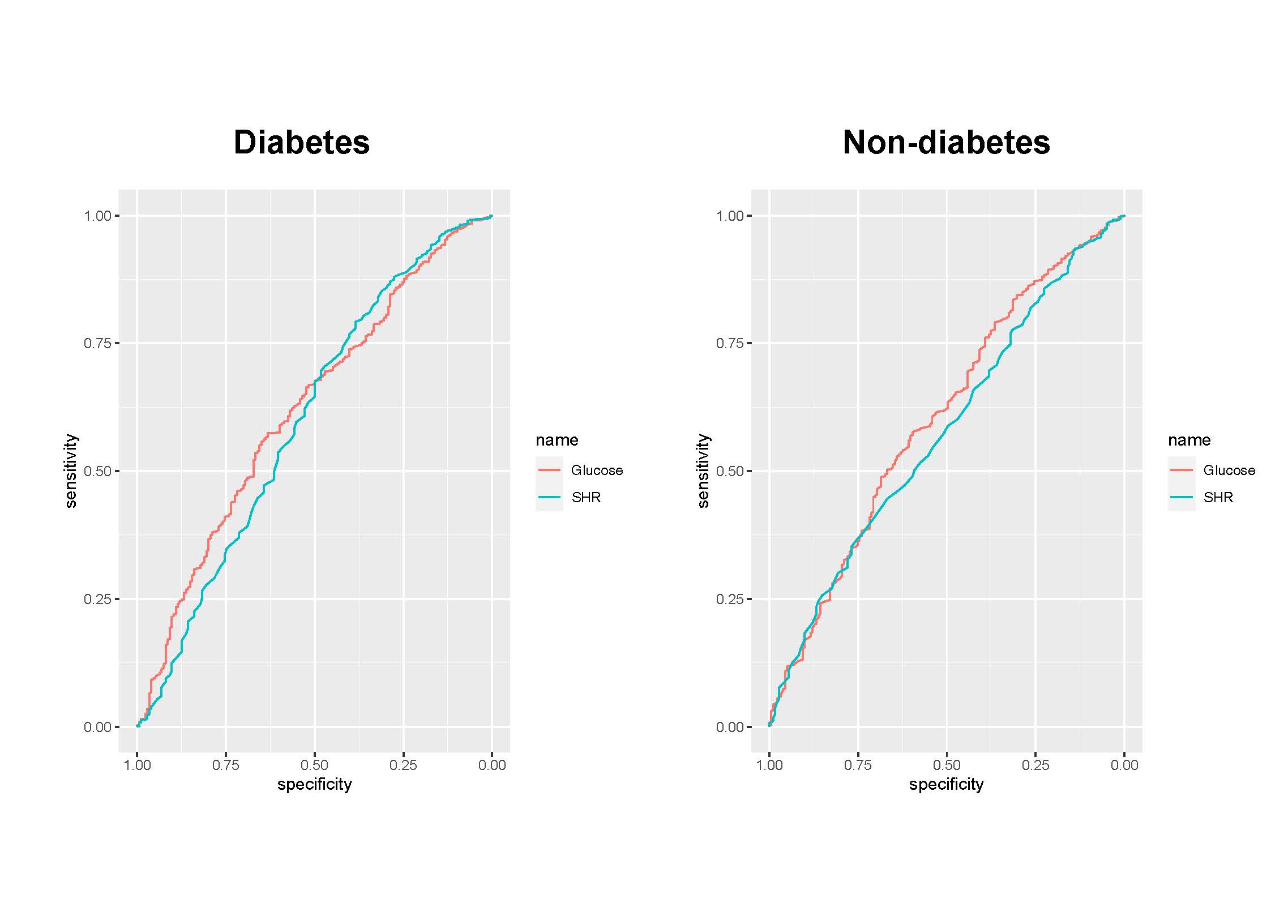
After multivariable adjustment, the highest tertiles of SHR and admission glucose were both significantly associated with an increased long-term mortality risk irrespective of diabetic status in patients with AMI. According to restricted cubic spline curves, positive linear associations between admission glucose and risk of long-term mortality were observed in subjects with diabetes and without diabetes (Figure 1). In contrast, the association between SHR and long-term mortality appeared to be J-shaped in patients with diabetes (Figure 1). The area under curves (AUC) for admission glucose were higher than AUC for SHR in both diabetic (0.621 vs. 0.599) and non-diabetic patients (0.597 vs. 0.566) (Figure 2).
Conclusion
Elevated admission glucose and stress hyperglycemia ratio were both significantly associated with the long-term mortality risk. Compared with admission glucose, stress hyperglycemia ratio has no superiority in long-term mortality prediction of AMI patients.