
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-035
Fractional Flow Reserve in Left Main Bifurcation From a Single Fluoroscopic View Versus Computed Tomography
By Nozomi Kotoku, Daixin Ding, Kai Ninomiya, Neil O’Leary, William Wijns, Shengxian Tu, Nicolo Piazza, Yoshinobu Onuma, Patrick W. Serruys
Presenter
Nozomi Kotoku
Authors
Nozomi Kotoku1, Daixin Ding1, Kai Ninomiya2, Neil O’Leary1, William Wijns1, Shengxian Tu3, Nicolo Piazza4, Yoshinobu Onuma1, Patrick W. Serruys1
Affiliation
University of Galway, Ireland1, Iwate Medical University, Japan2, Shanghai Jiao Tong University, China3, McGill University Health Center, Canada4
View Study Report
TCTAP A-035
Bifurcation/Left Main Diseases and Intervention
Fractional Flow Reserve in Left Main Bifurcation From a Single Fluoroscopic View Versus Computed Tomography
Nozomi Kotoku1, Daixin Ding1, Kai Ninomiya2, Neil O’Leary1, William Wijns1, Shengxian Tu3, Nicolo Piazza4, Yoshinobu Onuma1, Patrick W. Serruys1
University of Galway, Ireland1, Iwate Medical University, Japan2, Shanghai Jiao Tong University, China3, McGill University Health Center, Canada4
Background
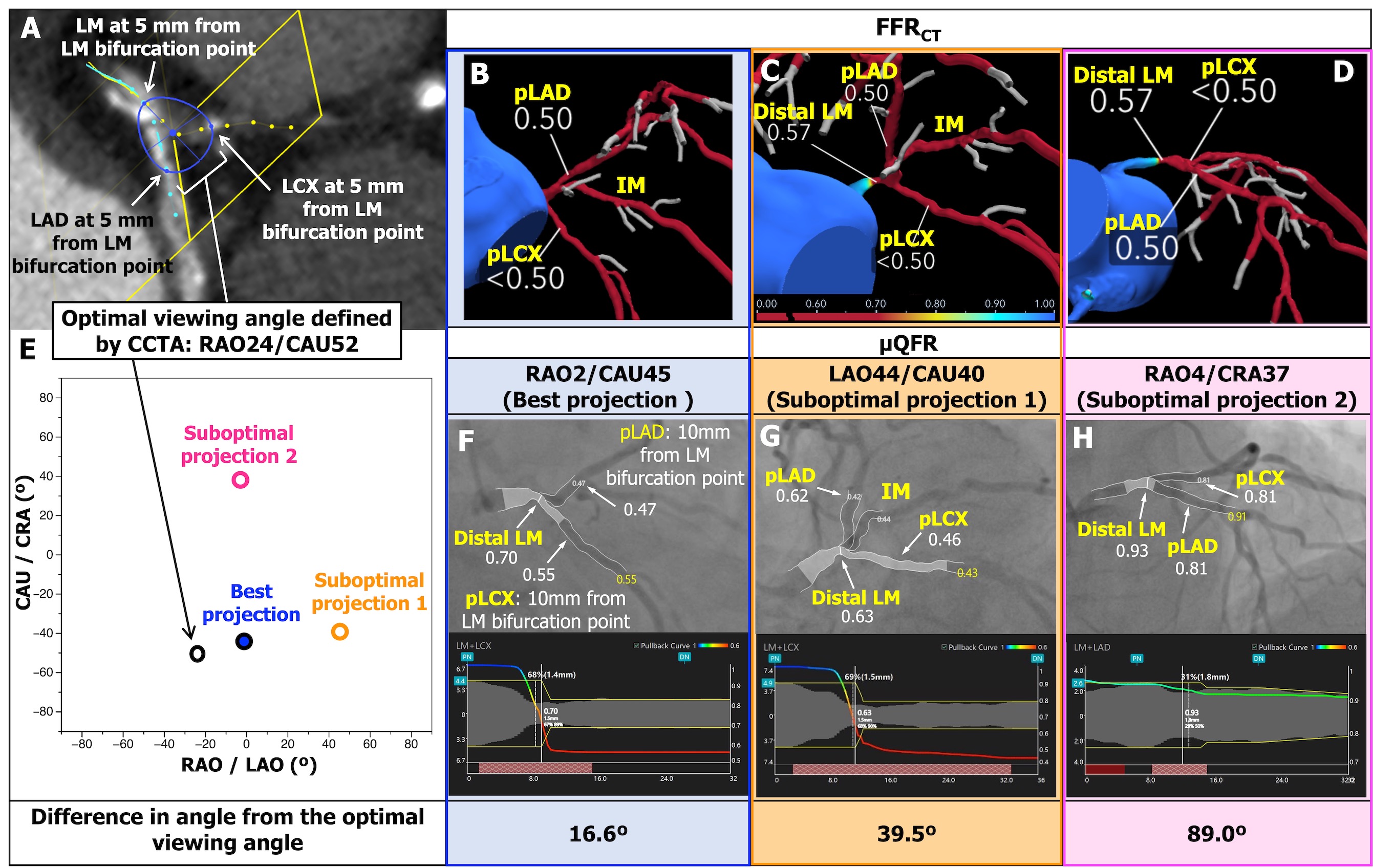
Murray law-based quantitative flow ratio (µQFR) assesses fractional flow reserve (FFR) in bifurcation lesions using a single angiographic view, enhancing the feasibility of analysis; however, accuracy may be compromised in suboptimal angiographic projections. FFRCT is a well-validated non-invasive method of measuring FFR from coronary computed tomographic angiography (CCTA). We evaluated the feasibility of µQFR in left main (LM) bifurcations, the impact of the optimal/suboptimal fluoroscopic view with respect to CCTA, and its diagnostic concordance with FFRCT.
Methods
In 300 patients with three-vessel disease, the values of FFRCT and µQFR were compared at the distal LM, proximal left anterior descending artery (pLAD) and circumflex artery (pLCX) (Figure 1). The optimal viewing angle of the LM bifurcation was defined on CCTA by 3-dimensional coordinates and converted into a 2-dimensional fluoroscopic view. The best fluoroscopic projection was considered the closest angulation to the optimal viewing angle on CCTA.
Results
µQFR was successfully computed in 805 projections. The prevalence of FFRCT ≤ 0.80 was 5.3%, 17.3%, and 15.3% in the distal LM, pLAD, and pLCX, respectively. In the best fluoroscopic projections, µQFR sensitivity was 86.5% (95% confidence interval [CI]: 74.2 - 94.4) and 80.4% (95% CI: 66.1 - 90.6), and specificity was 96.8% (95% CI: 93.7 - 98.6) and 96.9% (95% CI: 93.9 - 98.6), with regard to FFRCT of pLAD and pLCX. The AUC of µQFR for predicting an FFRCT ≤ 0.80 was improved using the best versus suboptimal projections (0.94 vs. 0.89, p = 0.027).
Conclusion
Computation of µQFR in LM bifurcations using a single angiographic view has high feasibility. Since the angiographic view influences the result of µQFR, CCTA may in advance identify the best angiographic projection to optimize the calculation of µQFR.