
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-081
Reducing Radiation Dose in Coronary Angiography and Angioplasty Using Dose Reduction Protocol
By Amitabh Yaduvanshi, Ishita Yaduvanshi, Mohit M Bhagwati, Vikas Kataria
Presenter
Ishita Yaduvanshi
Authors
Amitabh Yaduvanshi1, Ishita Yaduvanshi2, Mohit M Bhagwati1, Vikas Kataria1
Affiliation
Holy Family Hospital, India1, Baba Saheb Ambedkar Medical College and Hospital, India2
View Study Report
TCTAP A-081
Others (Unclassified)
Reducing Radiation Dose in Coronary Angiography and Angioplasty Using Dose Reduction Protocol
Amitabh Yaduvanshi1, Ishita Yaduvanshi2, Mohit M Bhagwati1, Vikas Kataria1
Holy Family Hospital, India1, Baba Saheb Ambedkar Medical College and Hospital, India2
Background
This study sought to quantitatively evaluate the reduction of radiation dose in coronary angiography and angioplasty with the use of theDose Reduction Protocol (DRP) in routine clinical settings.
Methods
A Dose Reduction Protocol during coronary interventions was implemented at a tertiary care hospital in September 2018 which included lowering the Fluoroscopy frame rates from 15 fps to 8 fps, frequent use of ‘flurosave’, and decreasing the cine frame rate from 15fps to 10fps. Radiation exposure data for all coronary procedures done using DRP at a tertiary care hospital between October 2018 to November 2020 were collected. For comparison, radiation dose data from consecutive coronary procedures performed without DRP in the same center from April 2015 to September 2018 were evaluated. Data was segregated into diagnostic coronary angiography (CAG) and single-vessel Percutaneous Intervention (PCI). The parameters collected include fluoroscopy time, dose area product (PKA), skin surface entry dose(KAR), and fluoroscopy time (FT).
Results
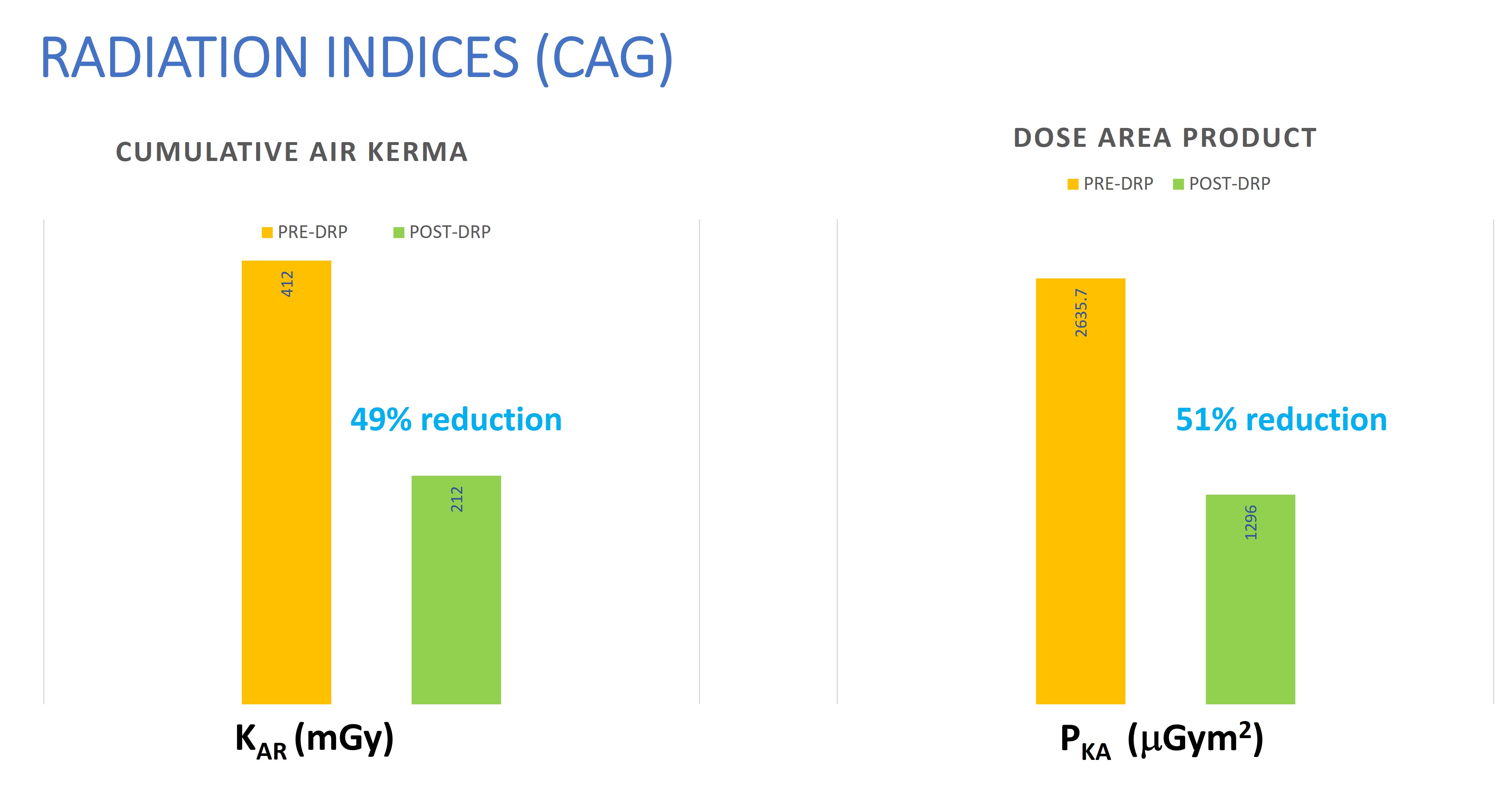
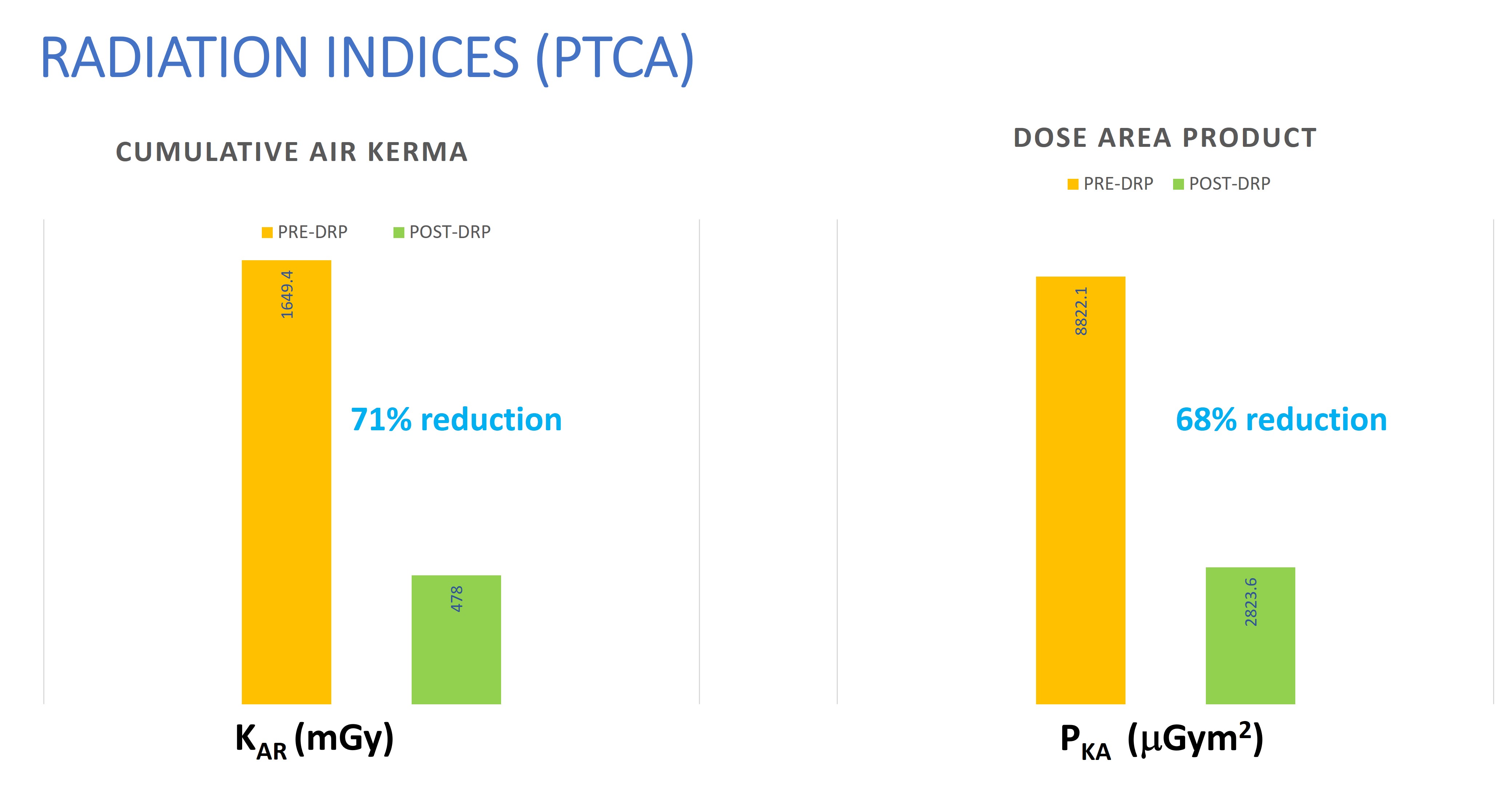
There were no significant differences between the 2 evaluated groups in gender, age, and weight. The median fluoroscopy time during coronary angiography was 2.4 min and 2.7 min in the two groups, and for single vessel angioplasty, it was 8.5 min and 9.3 min in both groups (not significant). The median dose area product was reduced from 2635.7 to 1296 mGym2 (51%, p <0.001) in coronary angiograms and from 8822.1 to 2823 mGym2 (68%, p <0.001) in single vessel coronary interventions using the DRP. The median skin surface entrance dose was reduced from 412 to 212 mGy (49%, p <0.001) in coronary angiograms and from 1649 to 478 mGy (71%, p <0.001) in single vessel coronary interventions using the Dose reducing Protocol. Image quality was graded as similar between the evaluated periods (4.0 vs 4.2, not significant).
Conclusion
By using a Dose Reducing Protocol, where the fluoroscopy frame rate is decreased to 8fps and the cine frame rate is decreased to 10fps, a substantial reduction in radiation exposure could be achieved without the need to prolong the procedure or fluoroscopy time. The image quality did not decrease significantly and clinically useful images were obtained using the dose-reducing protocol. In accordance with the ALARA principle of radiation exposure, a reduced frame rate, frequent use of the fluoro-save feature and reduced use of cine should be incorporated in all cath lab intervention procedures.