Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-075
Asymptomatic Left Ventricular Dysfunction in Patients With or Without Type 2 Diabetic Mellitus: A Population-Based Cohort Study
By Lo-Chieh Ling, Shih-Hsien Sung, Chern-En Chiang
Presenter
Lo-Chieh Ling
Authors
Lo-Chieh Ling1, Shih-Hsien Sung2, Chern-En Chiang1
Affiliation
Taipei Veterans General Hospital, Taiwan1, National Yang Ming Chiao Tung University, Taiwan2
View Study Report
TCTAP A-075
Diabetes
Asymptomatic Left Ventricular Dysfunction in Patients With or Without Type 2 Diabetic Mellitus: A Population-Based Cohort Study
Lo-Chieh Ling1, Shih-Hsien Sung2, Chern-En Chiang1
Taipei Veterans General Hospital, Taiwan1, National Yang Ming Chiao Tung University, Taiwan2
Background
Type 2 diabetes mellitus (T2DM) has been related toventricular systolic and diastolic dysfunction and subsequent heart failure.The study aimed to investigate the prevalence of asymptomatic left ventriculardysfunction (aLVD) in subjects with T2DM, and its predisposing factors.
Methods
Subjects without existed cardiovascular disease wereeligible for this study. Left ventricular ejection fraction (LVEF), mitral E/Aratio, peak mitral annulus tissue velocity (e’), left atrial dimension (LAD),peak tricuspid regurgitation velocity (TR Vmax) were obtained by a standardechocardiographic study. Asymptomatic left ventricular diastolic dysfunction(ALVSD) was defined as LVEF< 50% and the asymptomatic left ventriculardiastolic dysfunction (ALVDD) was defined as having three or more of the fourparameters: septal e' < 7, septal E/e’>15, LAD > 40mm, and TR Vmax> 2.8 m/s. All-cause mortality up to 2 years wasobtained by linking to the National Death Registry.
Results
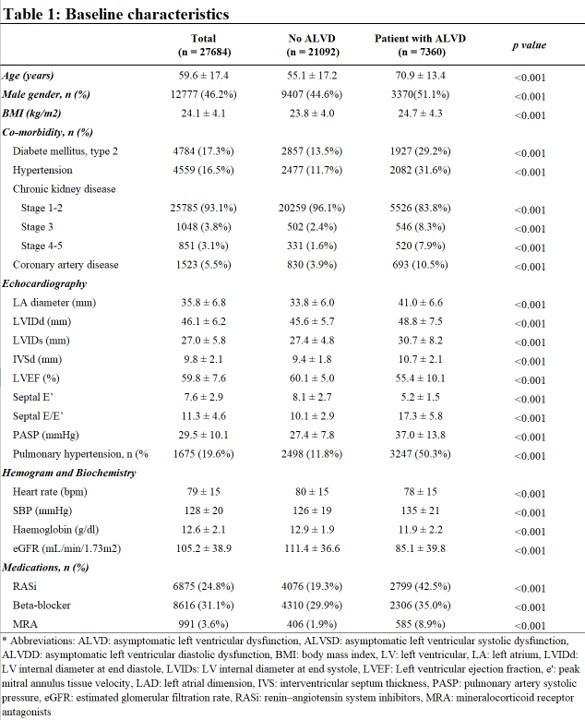
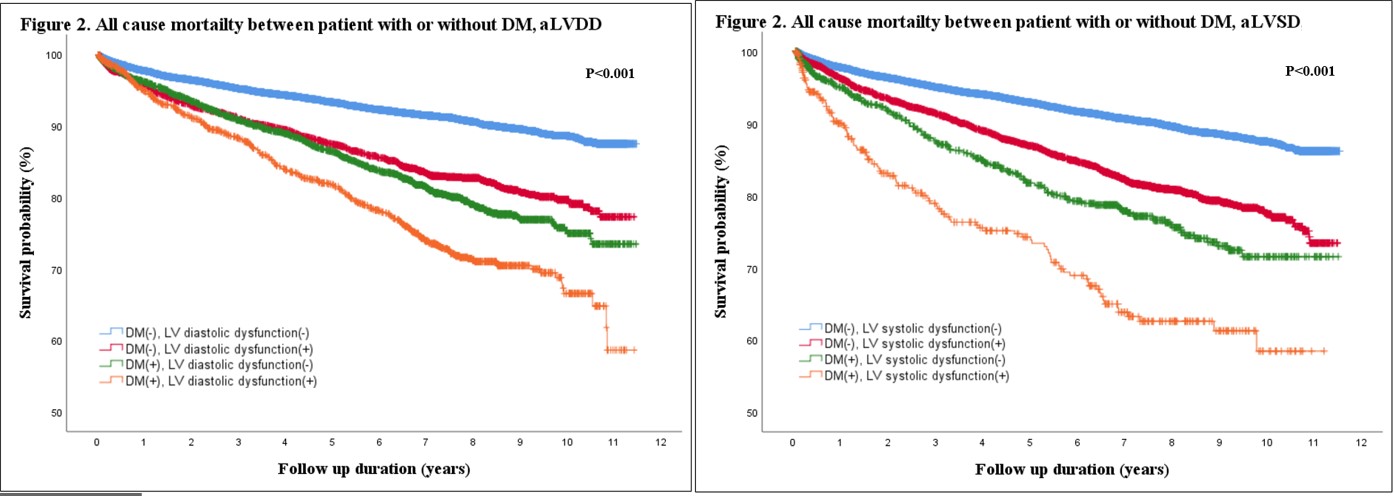
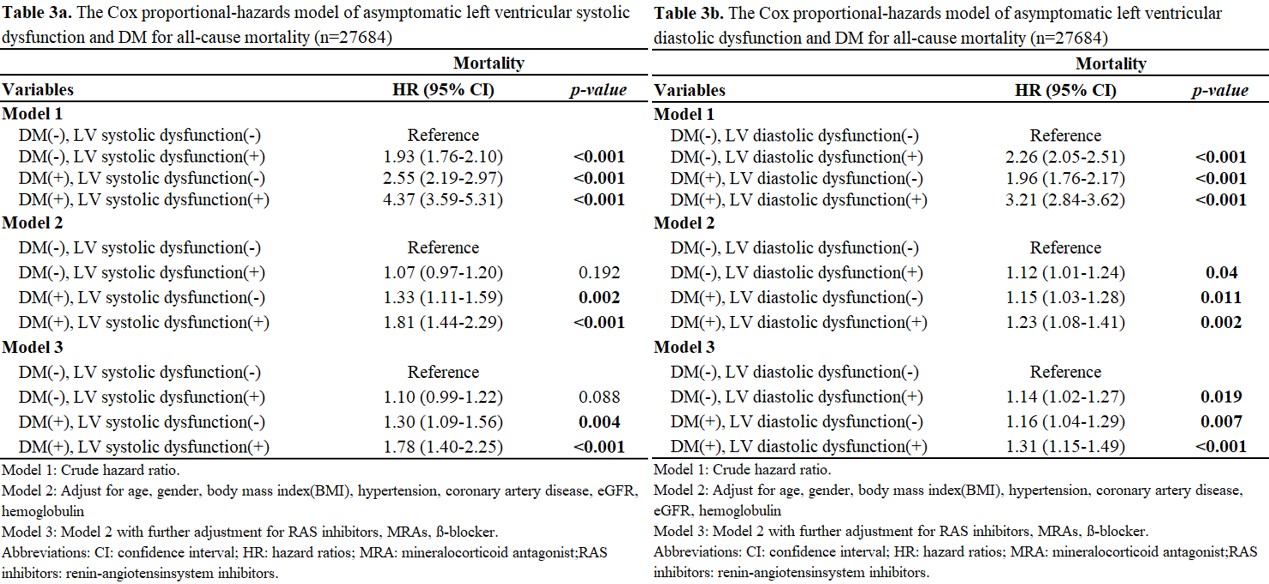
A total of 27684 subjects (59.6±17.4 years, 46.2% men, 17.7%diabetes) were included in this study(Table 1). The ALVSD patientswere older, male dominant, more prevalent with hypertension, diabetes mellitusand coronary artery disease, and had higher BMI, lower hemoglobin, andestimated glomerular filtration rate. ALVSD and ALVDD was more prevalent inpatients with T2DM than those without (4.9% vs 8.2%, P<0.001)(15.4% v.s.32.1%) (Figure 1). Age (odds ratio and 95% confidence interval: 1.04, 1.03–1.04), male gender(2.24, 1.99-2.52), T2DM (1.28, 1.11-1.46), coronary artery disease (1.38,1.14-1.68), hemoglobin (0.95, 0.91-1.00), CKD stage 3(2.02, 1.63-2.50), and CKD stage 4-5(3.95,3.06-5.09) were all independently correlated toALVSD(Table 2a). Onthe other hand age (odds ratio and 95% confidenceinterval: 1.07, 1.07–1.08), BMI (1.12, 1.11-1.13), T2DM (1.34, 1.24-1.46), hypertension (1.31, 1.20-1.43), hemoglobin (0.88, 0.85-0.91), and CKD stage 4-5(3.11, 2.58-3.76) were independently correlated to ALVDD(Table 2b). During a mean follow-upof 5.3 ± 3.6 years, there were 2625 deaths (9.5%). The Kaplan–Meier curveanalysis revealed diabetic subjects with were associated with the worstsurvival rate than those with either T2DM or ALVSD/ALVDD (Figure 2). TheCox regression analysis revealed the ALVDD and ALVSD was related to mortality,independent of age, gender, body mass index, hypertension, coronary arterydisease, hemoglobulin, estimated glomerular filtration rate, and medication[hazard ratio and 95% confidence interval of mortality(ALVSD/ALVDD): 1.78(1.40–2.25)/1.31(1.15-1.49)].