
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-028
Ethnic Differences in Left Main Coronary Artery Diameter
By Abdul Rahman Arabi, Ihsan Rafie, Abid Khan, Manoj Montu Almeida, Sara Karam Al-Balushi
Presenter
Abid Khan
Authors
Abdul Rahman Arabi1, Ihsan Rafie2, Abid Khan2, Manoj Montu Almeida1, Sara Karam Al-Balushi2
Affiliation
Hamad Medical Corporation, Qatar1, Hamad Medical Corporation (HMC), Doha, Qatar2
View Study Report
TCTAP A-028
Bifurcation/Left Main Diseases and Intervention
Ethnic Differences in Left Main Coronary Artery Diameter
Abdul Rahman Arabi1, Ihsan Rafie2, Abid Khan2, Manoj Montu Almeida1, Sara Karam Al-Balushi2
Hamad Medical Corporation, Qatar1, Hamad Medical Corporation (HMC), Doha, Qatar2
Background
Background : Most cardiac catheterization laboratories use a single cut-off value (minimal lumen area < 6 mm² ) to identify significant Left Main Coronary Artery (LMCA) disease on intravascular imaging. This approach assumes all ethnic groups have similar LMCA diameters. The accuracy of this assumption incenters with a multi-racial cohort is unknown. This study compared the left main artery diameter of South Asian and Arabic patients.
Methods
Methods : We measured the Left Main Coronary Artery (LMCA) diameter using a Quantitative Coronary Angiogram (QCA) in consecutive patients who underwent coronary angiogram for various clinical indications and had angiographically normal LMCA. We compared the diameter in South Asian (SA) Vs. Arab patients in the anterior-posterior caudal and anterior-posterior cranial views.
Results
Results : One hundred eighty-eight patients (121 SA and 67 Arabs) were enrolled. SA patients were younger with a lower Body Mass Index (BMI) and Body Surface Area (BSA). Diabetes, hypertension, and tobacco use were similar in the two groups (Table1). In the anterior-posterior cranial view, the LMCA diameter was significantly smaller among SA (4.25 +/-0.70 mm) than Arabs (4.54 +/- 0.80 mm, P= 0.00In the anterior-posterior caudal view, the LMCA diameter was numerically smaller among SA (4.37+/- 0.75 vs. 4.60+/- 0.81 mm, P=0.053). South Asian ethnicity, diabetes, and BSA were associated with a smaller LMCA diameter. However, in the multiple linear regression, race and diabetes were the only factors associated with a smaller LMCA diameter (p= 0.031 and p= 0.014)
Table 1:Demographic of patients
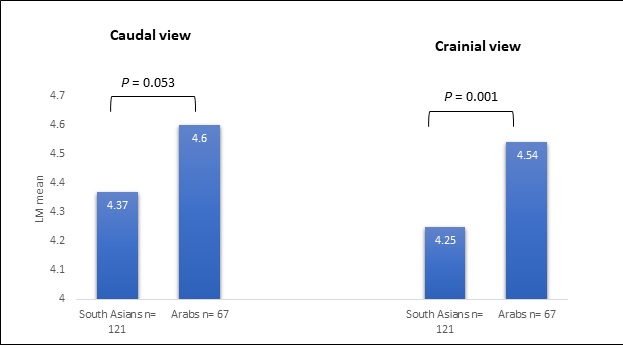
Table 1:Demographic of patients
| South Asians | Arabs | P-value | |
| Demographics | |||
| Age (Mean,SD) | 48 (8.55) | 55 (9.57) | <0.001 |
| Men | 120 (99%) | 47 (70%) | <0.001 |
| BSA (Median, IQR) | 1.8 (0.2) | 1.89 (0.32) | <0.001 |
| BMI (Median, IQR) | 26.13 (4.58) | 28.98 (6.75) | <0.001 |
| DM | 54 (45 %) | 33 (49%) | 0.72 |
| HTN | 46 (38%) | 33 (49%) | 0.32 |
| Smoker | 39 (32%) | 21 (31%) | 0.87 |
Conclusion
Conclusion : We observed significant ethnic differences in LMCA diameter, which might necessitate ethnic-specific cut-off in the catheterization laboratories with mixed-patient populations.