
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-070
Non-Invasive Assessment of Microvascular Dysfunction After Optimal Coronary Artery Stent Deployment; Insight From Acetyl Salicylic Elimination Trial (Aset) Japan
By Patrick W. Serruys, Shinichiro Masuda, Shigetaka Kageyama, Kai Ninomiya, Nozomi Kotoku, Pruthvi Revaiah, Yoshinobu Onuma
Presenter
Patrick W. Serruys
Authors
Patrick W. Serruys1, Shinichiro Masuda1, Shigetaka Kageyama1, Kai Ninomiya2, Nozomi Kotoku1, Pruthvi Revaiah1, Yoshinobu Onuma1
Affiliation
University of Galway, Ireland1, Iwate Medical University, Japan2
View Study Report
TCTAP A-070
Physiologic Lesion Assessment
Non-Invasive Assessment of Microvascular Dysfunction After Optimal Coronary Artery Stent Deployment; Insight From Acetyl Salicylic Elimination Trial (Aset) Japan
Patrick W. Serruys1, Shinichiro Masuda1, Shigetaka Kageyama1, Kai Ninomiya2, Nozomi Kotoku1, Pruthvi Revaiah1, Yoshinobu Onuma1
University of Galway, Ireland1, Iwate Medical University, Japan2
Background
Angiography-derived index of microcirculatory resistance (IMR) is a non-invasive, alternative tool for invasive IMR measurement. Reports on angio-IMR immediately after optimal stenting are limited.
Methods
This is a sub-study of the ASET-Japan trial that assesses the safety and feasibility of low-dose prasugrel monotherapy (3.75 mg/day) after successful everolimus-eluting stent(s) deployment for patients with CCS or NSTE-ACS. All the patients are enrolled after achieving optimal stent implantation with intravascular imaging guidance in 88.4% of the stents. We assess angiography-derived IMR calculated with the following formula:(Pa–[0.1*Pa]) *QFR* (vessel length/Vhyp) (where Vhyp is an estimation of hyperemic flow velocity). High IMR was defined as a measurement ≥25 units.
Results
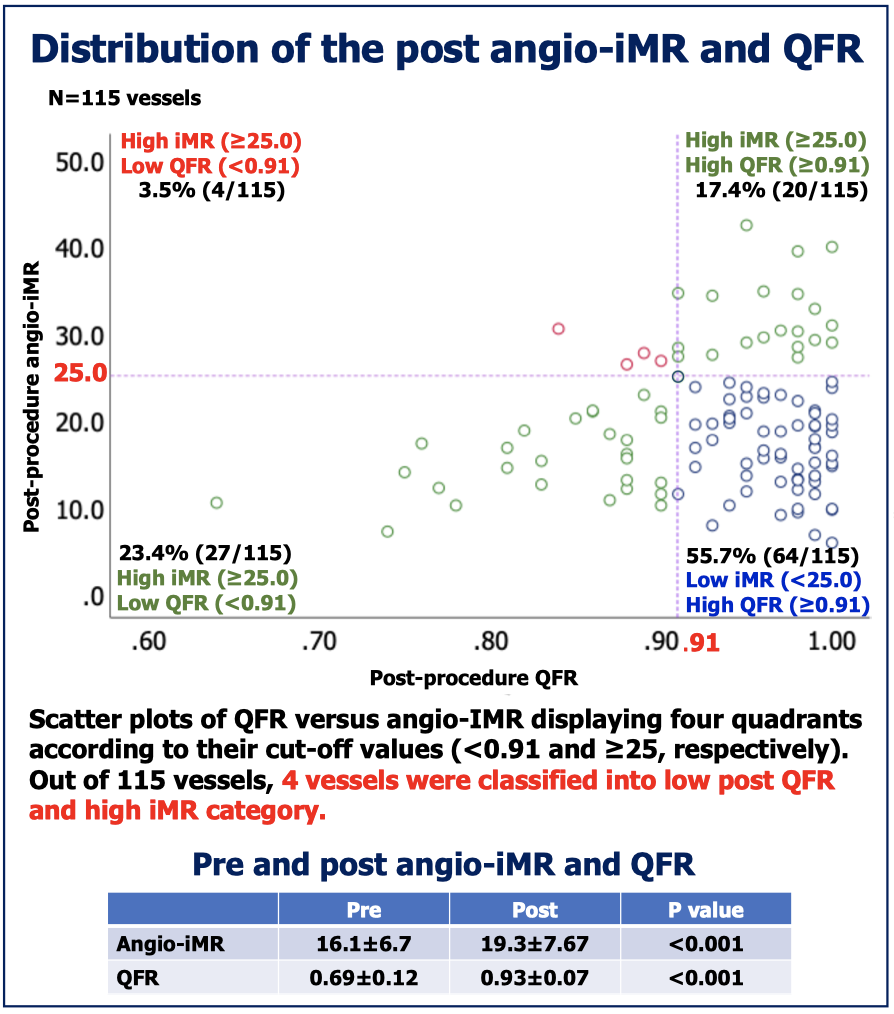
Post- and pre-procedural QFR/IMRs are evaluated in 115 treated vessels in 112 patients with 24.1% of CCS and 75.9% of NSTE-ACS. Mean age is 68.6 ± 9.8, 88.4% are male and the incidence of diabetes is 32.1%. As shown in the figure, both post-procedural QFR and IMR are significantly higher than pre-procedure. Post-procedural IMR≥25 is documented in 24 vessels (20.9%). As we apply the post-QFR cut-off value of 0.91, 55.7% of the vessels are categorized into low IMR /high QFR groups. Only 4 vessels (3.5%) are categorized into high IMR/low-QFR category.
Conclusion
In this prospective study with optimal stent results, 4 coronary hemodynamic profiles emerge. The clinical and anginal repercussions of these profiles will be evaluated at follow-up.