
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-103
A Case Series of Snare-Assisted Transcatheter Aortic Valve Implantation in Challenging Anatomy
By Kar Lok Leo Lai, Kevin Ka-Ho Kam, Ka Lung Chui, Randolph Hung-Leung Wong, Alex, Pui Wai Lee, Eugene Brian Wu, Kent, Chak Yu So
Presenter
Kar Lok Leo Lai
Authors
Kar Lok Leo Lai1, Kevin Ka-Ho Kam1, Ka Lung Chui1, Randolph Hung-Leung Wong1, Alex, Pui Wai Lee1, Eugene Brian Wu1, Kent, Chak Yu So2
Affiliation
Prince of Wales Hospital, Hong Kong, China1, Prince Of Wales Hospital, Chinese University of Hong Kong, Hong Kong, China2
View Study Report
TCTAP A-103
Valvular Intervention: Aortic
A Case Series of Snare-Assisted Transcatheter Aortic Valve Implantation in Challenging Anatomy
Kar Lok Leo Lai1, Kevin Ka-Ho Kam1, Ka Lung Chui1, Randolph Hung-Leung Wong1, Alex, Pui Wai Lee1, Eugene Brian Wu1, Kent, Chak Yu So2
Prince of Wales Hospital, Hong Kong, China1, Prince Of Wales Hospital, Chinese University of Hong Kong, Hong Kong, China2
Background
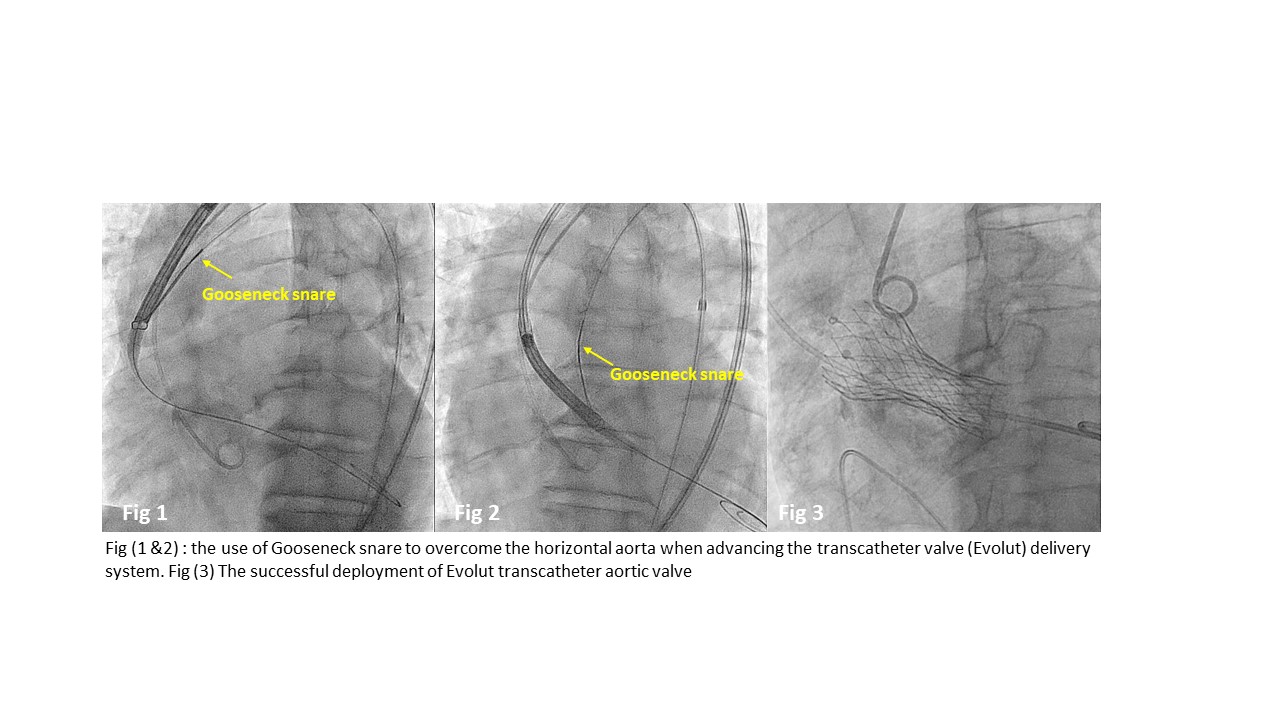
Transcatheter aortic valve implantation is widely used for treating severe aortic stenosis. Self-expanding valve including the Evolut family has lower root complications in patients with severely calcified aortic complex. However, Evolut Implantation could be more challenging in the presence of a dilated aortic root and horizontal aorta. We hypothesized that the use of Snare-assisted technique can overcome these challenges by centralizing the system to facilitate valve crossing, and hence improve the safety and efficiency of the procedure.
Methods
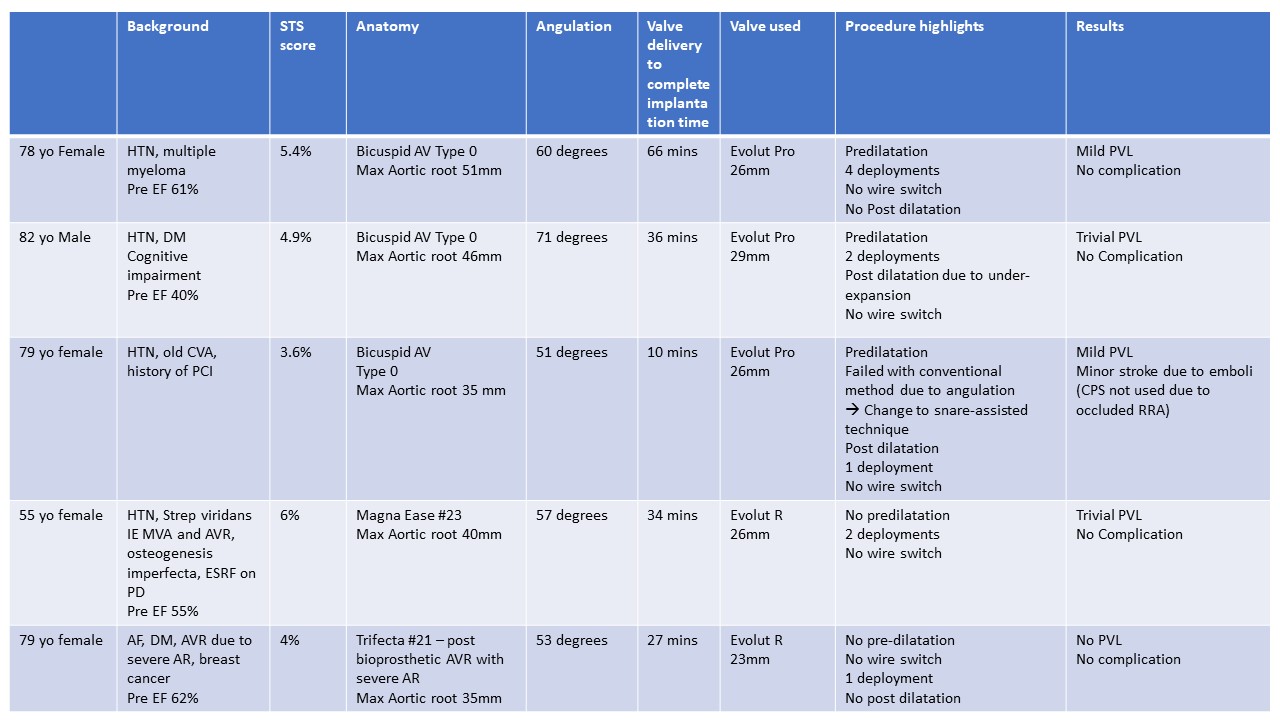
We performed a retrospective analysis of TAVI in challenging aortic anatomy using the Snare-assisted technique from 2021 to 2022. The numbers of self-expanding aortic valve used were identified. Different parameters including the STS score, anatomy of the aortic valve and angulation of the aorta were reviewed. We measured the time required from advancement of the TAVI delivery system to deployment of the transcatheter valve and assess each case individually.
Results
Five patients were identified. Three of them had type 0 bicuspid aortic valve and the other two had bioprosthetic valve failure. All of them had severe aortic stenosis except the Trifecta failure had severe aortic regurgitation. The Society of Thoracic Surgeons Scores (STS) were between 3.6 to 6%. The maximum aortic root sizes were between 35 to 51mm. The angulations of the aorta were ranging from 51 to 71 degrees. The procedural time from advancing the valve to the deployment of valve were between 10 to 66 minutes. LV wire switch was not required with the use of Snare. One case (51 degrees angulation of aorta) required the switch from conventional method to Snare technique after failed to advance the valve due to severe angulation and wire bias. After using the Snare-assisted technique, the deployment time was minimized to 10 minutes only. The follow up echocardiography did not show any significant paravalvular leak and all of them have improved NYHA classification. These cases demonstrated that the use of Snare technique could reduce the time duration of valve crossing and minimize the force applied to cross the native valve, and hence lowering the risk of annular or aortic root injury.
Conclusion
These five cases have demonstrated the use of snare-assisted technique in TAVI using self-expanding valve has good procedural safety and efficiency in challenging aortic root anatomy.