Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-066
Agreement Between Different Angiography-Derived Modalities With Wire-Based Fractional Flow Reserve Systems and 30 Month Clinical Outcomes in Evaluation of Non-Hemodynamically Significant Obstructive Coronary Artery Disease, a Single Centre Experience
By Han Bing Chow, Chandan Deepak Bhavnani, Kian Hui Ho, Chen Ting Tan, Francis Shu, Keng Tat Koh, Yen Yee Oon, Asri Bin Said, Alan Fong, Tiong Kiam Ong
Presenter
Han Bing Chow
Authors
Han Bing Chow1, Chandan Deepak Bhavnani2, Kian Hui Ho3, Chen Ting Tan3, Francis Shu3, Keng Tat Koh3, Yen Yee Oon3, Asri Bin Said4, Alan Fong3, Tiong Kiam Ong3
Affiliation
Tuen Mun Hospital, Hong Kong, China1, Hospital Serdang, Malaysia2, sarawak heart centre, Malaysia3, Universiti Malaysia Sarawak, Malaysia4
View Study Report
TCTAP A-066
Physiologic Lesion Assessment
Agreement Between Different Angiography-Derived Modalities With Wire-Based Fractional Flow Reserve Systems and 30 Month Clinical Outcomes in Evaluation of Non-Hemodynamically Significant Obstructive Coronary Artery Disease, a Single Centre Experience
Han Bing Chow1, Chandan Deepak Bhavnani2, Kian Hui Ho3, Chen Ting Tan3, Francis Shu3, Keng Tat Koh3, Yen Yee Oon3, Asri Bin Said4, Alan Fong3, Tiong Kiam Ong3
Tuen Mun Hospital, Hong Kong, China1, Hospital Serdang, Malaysia2, sarawak heart centre, Malaysia3, Universiti Malaysia Sarawak, Malaysia4
Background
Coronary physiology assessment of non-flow limiting stensoses is recommended in contemporary guidelines inpatients with stable coronary artery disease (CAD). Application of computational fluid dynamics to derive fractional flow reserve (FFR) eliminates the potential complications associated with hyperemia and introduction of pressure sensor wires into the coronary arteries. Angiography-derived FFR has shown consistent accuracy with wire-based systems in lesion selection for percutaneous coronary intervention (PCI). To date, comparison between different angiography-derived FFR systems has not been performed, particularly in the subset of patients with non-hemodynamically significant CAD, where PCI was deferred.
We aim to assess the agreement between different wire-free FFR systems (coronary angiography-derived fractional flow reserve (CAFFR) and quantitative flow ratio (QFR)) with wire-based FFR and the associated 30-month clinical outcomes of PCI deferral. The primary end point was a composite of death from any cause, myocardial infarction (MI) or target vessel revascularization (TVR).
We aim to assess the agreement between different wire-free FFR systems (coronary angiography-derived fractional flow reserve (CAFFR) and quantitative flow ratio (QFR)) with wire-based FFR and the associated 30-month clinical outcomes of PCI deferral. The primary end point was a composite of death from any cause, myocardial infarction (MI) or target vessel revascularization (TVR).
Methods
A prospective, single centre study was conducted from December 2019 to June 2020 involving 69 patients (93vessels) with angiographic stenosis of 30%-90%. After excluding patients with CAFFR of <0.80 or poor-quality images, data from 29 patients (31 vessels) were analysed. Wire-based FFR was performed in 14 patients (48%) for comparison, at the operator’s discretion. QFR analysis was carried out offline on patients with 2 angiographic views 25 degree apart to compare respective values.
Results
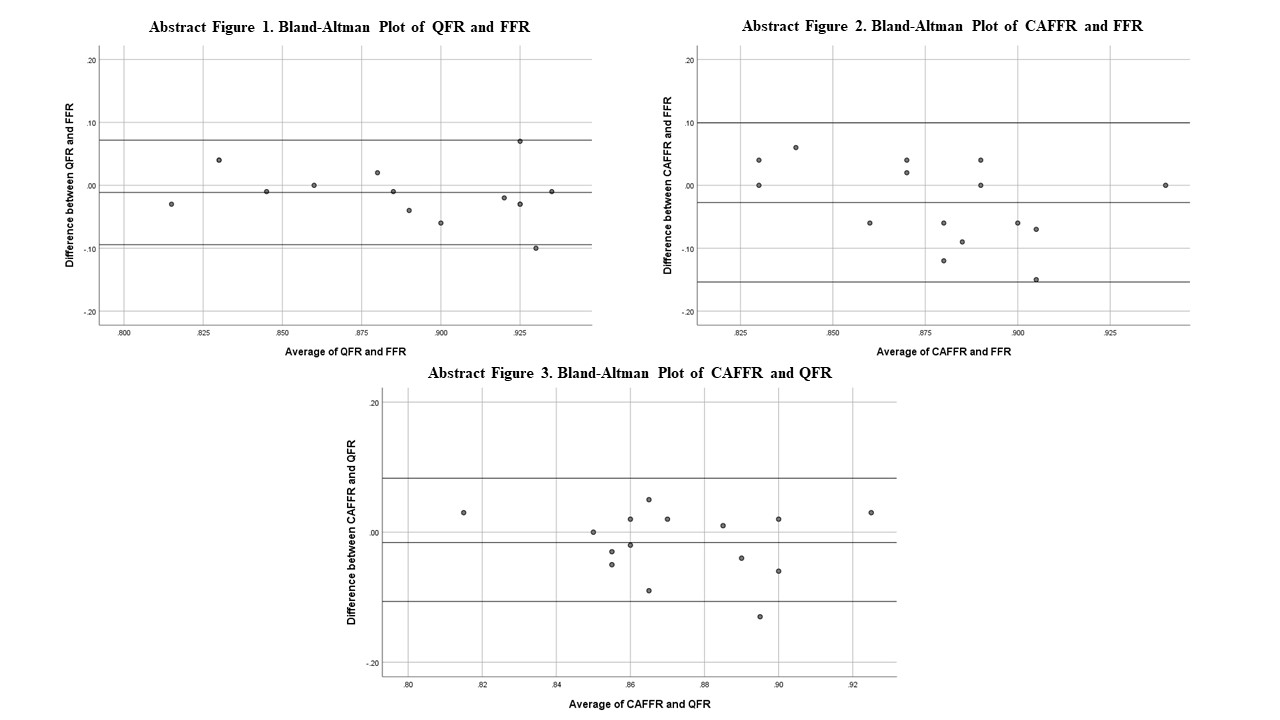
Among the study cohort, 83% were male. The mean age was 59 ± 12.6 years old. 12 (41%) patients were diabetic, 18 (62%) were hypertensive, 17 (59%) had dyslipidemia and 18 (62%) had a smoking history. The mean LVEF was 52+/-11.4%. 22 (76%) of the patients had a recent acute coronary syndrome. LAD artery was assessed in 16 (52%) vessels. The mean CAFFR, FFR and QFR was 0.80 ± 0.05, 0.89 ± 0.05 and 0.83 ± 0.05 respectively. In the Bland-Altman plots (abstract figure 1-3), there were no significant discrepancies between the values with narrow limits of agreement and there was no significant proportional bias. In general, all three modalities showed good correspondence in hemodynamically significant (<0.80) and non-significant values (>0.80). There were zero procedural complications from CAFFR measurement and similarly for QFR measurements which was conducted offline. At 30 months, all 29 patients were alive. 2 patient (6.8%) met the primary end point (TVR for angina). 89.6% (26) patients remained in CCS class 1 on follow up.
Conclusion
The 30-month outcome data illustrates the efficacy of PCI deferral utilizing non-wired based techniques that is comparable to the gold standard wired FFR. Future research with a larger sample size and longer follow-up is desired.