
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-024
Synergistic Coronary Artery Calcium Modification With Combined Atherectomy and Intravascular Lithotripsy
By Ting Wai Bernard Wong, Eugene Brian Wu, Bryan Ping-Yen Yan
Presenter
Bernard Wong
Authors
Ting Wai Bernard Wong1, Eugene Brian Wu2, Bryan Ping-Yen Yan3
Affiliation
North Shore Hospital, New Zealand1, Prince of Wales Hospital, Hong Kong, China2, The Chinese University of Hong Kong, Hong Kong, China3
View Study Report
TCTAP A-024
Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Synergistic Coronary Artery Calcium Modification With Combined Atherectomy and Intravascular Lithotripsy
Ting Wai Bernard Wong1, Eugene Brian Wu2, Bryan Ping-Yen Yan3
North Shore Hospital, New Zealand1, Prince of Wales Hospital, Hong Kong, China2, The Chinese University of Hong Kong, Hong Kong, China3
Background
Severe coronary artery calcification (CAC) remains challenging during percutaneous coronary intervention (PCI) and often requires one or more advanced calcium modification tools. We describe the combination use of rotational (RA) or orbital atherectomy (OA), with intravascular lithotripsy (IVL), termed Rotatripsy and Orbital-tripsy respectively, for modifying CAC prior to stent implantation during PCI.
Methods
Weperformed a retrospective analysis of patients treated with Rotatripsy orOrbital-tripsy at our center between July 2019 and March 2022. The primaryefficacy endpoint was procedural success (successful stent implantation,<30% residual stenosis visually, thrombolysis in myocardial infarction 3flow; absence of types C to F dissection/perforation or loss of side branch≥2.0mm visually) without in-hospital major adverse cardiovascular events (MACE,cardiovascular death, myocardial infarction [MI], target-vessel revascularization).
Following coronary angiography showingsignificant CAC and decision to proceed with PCI at the discretion of theinterventional cardiologist, intravascular imaging was performed. Opticalcoherence tomography (OCT) was performed with the Dragonfly OptisTMsystem (Abbott Vascular, SantaClara, CA, USA) and optical frequency domain imaging (OFDI) with the FastViewcatheter connected to the Lunawave® system (Terumo, Tokyo, Japan). Intravascularultrasound (IVUS) was performed with the Altaview catheter connected to theVISICUBE system (Terumo, Tokyo, Japan).
Following coronary angiography showingsignificant CAC and decision to proceed with PCI at the discretion of theinterventional cardiologist, intravascular imaging was performed. Opticalcoherence tomography (OCT) was performed with the Dragonfly OptisTMsystem (Abbott Vascular, SantaClara, CA, USA) and optical frequency domain imaging (OFDI) with the FastViewcatheter connected to the Lunawave® system (Terumo, Tokyo, Japan). Intravascularultrasound (IVUS) was performed with the Altaview catheter connected to theVISICUBE system (Terumo, Tokyo, Japan).
Results
A totalof 25 patients were included in our study (14 Rotatripsy and 11 Orbital-tripsy).The mean age was 72.2 ± 7.6 years and 76% were men. PCI was guided byintravascular imaging in 24 patients (96%). All cases were treated with either RA or OA before utilization of IVL. Procedural success was achieved in 22 cases (88%) with one side branch loss without peri-procedural MI (4%) and 2 in-patient deaths (8%) unrelated to the procedure (one intracranial hemorrhage and one cardiac arrest).
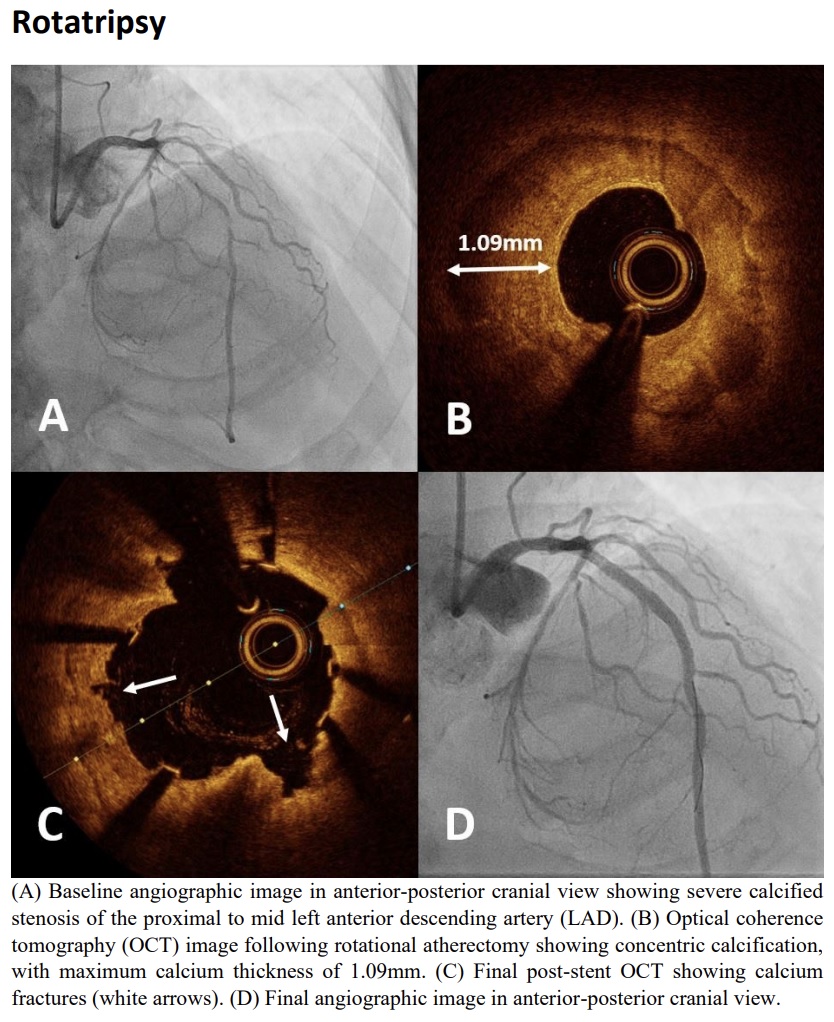
Rotatripsy
| Patient Characteristics | Patients (n=25) |
| Age, yrs. ± SD | 72.2 ± 7.6 |
| Male | 19 (76.0) |
| Hypertension | 23 (92.0) |
| Diabetes | 18 (72.0) |
| Dyslipidemia | 18 (72.0) |
| Previous stroke or TIA | 3 (12.0) |
| Smoking history | 9 (36.0) |
| Prior PCI | 12 (48.0) |
| Chronic kidney disease (eGFR <60mls/min/1.73m2) | 11 (44.0) |
| Presentation | 19 (76.0) |
Rotatripsy
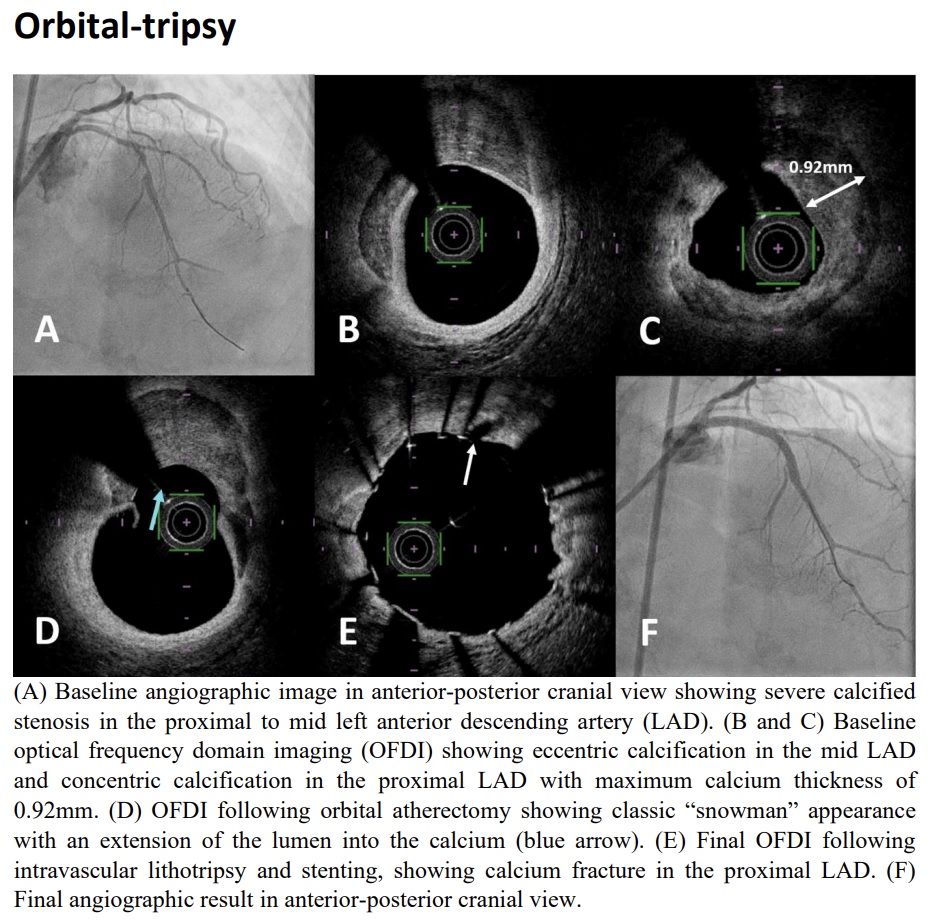
Orbital-tripsy
Conclusion
We describe efficacious use of both Rotatripsy and Orbital-tripsy to modify severe CAC during PCI in a real-world setting. Intravascular imaging can guide appropriate use of these devices to complement each other to modify severe CAC to achieve optimal outcomes.