
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-164
Cardiac MRI Sizing for Left Atrial Appendage Closure
By Joseph Reed, Luis Augusto Palma Dallan, Sadeer G Al-Kindi, Steven Filby
Presenter
Joseph Reed
Authors
Joseph Reed1, Luis Augusto Palma Dallan1, Sadeer G Al-Kindi1, Steven Filby1
Affiliation
University Hospitals Cleveland Medical Center, USA1,
View Study Report
TCTAP C-164
STRUCTURAL HEART DISEASE - Left Atrial Appendage Closure
Cardiac MRI Sizing for Left Atrial Appendage Closure
Joseph Reed1, Luis Augusto Palma Dallan1, Sadeer G Al-Kindi1, Steven Filby1
University Hospitals Cleveland Medical Center, USA1,
Clinical Information
Patient initials or Identifier Number
JH
Relevant Clinical History and Physical Exam
We describe an 82-year-old female with paroxysmal atrial fibrillation, prior stroke, heart failure with preserved ejection fraction, and advanced chronic kidney disease who was referred for LAAC due to gastrointestinal bleeding and gait instability with increased fall risk. Her CHA2DS2-VASc score was 6 and HAS-BLED score was 4. CTA was contraindicated due to a GFR of less than 30 mL/min/1.73m2. The patient did not tolerate transesophageal echocardiography due to dysphagia.
Relevant Test Results Prior to Catheterization
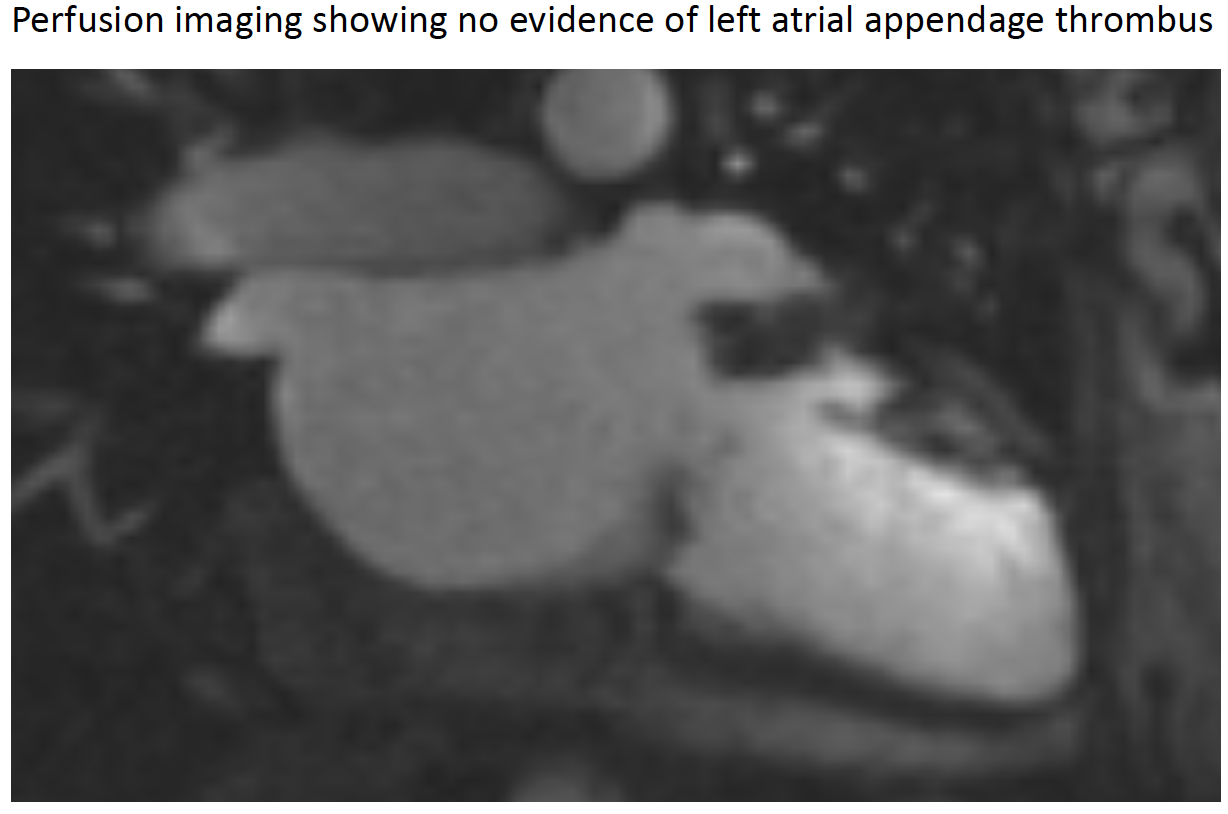
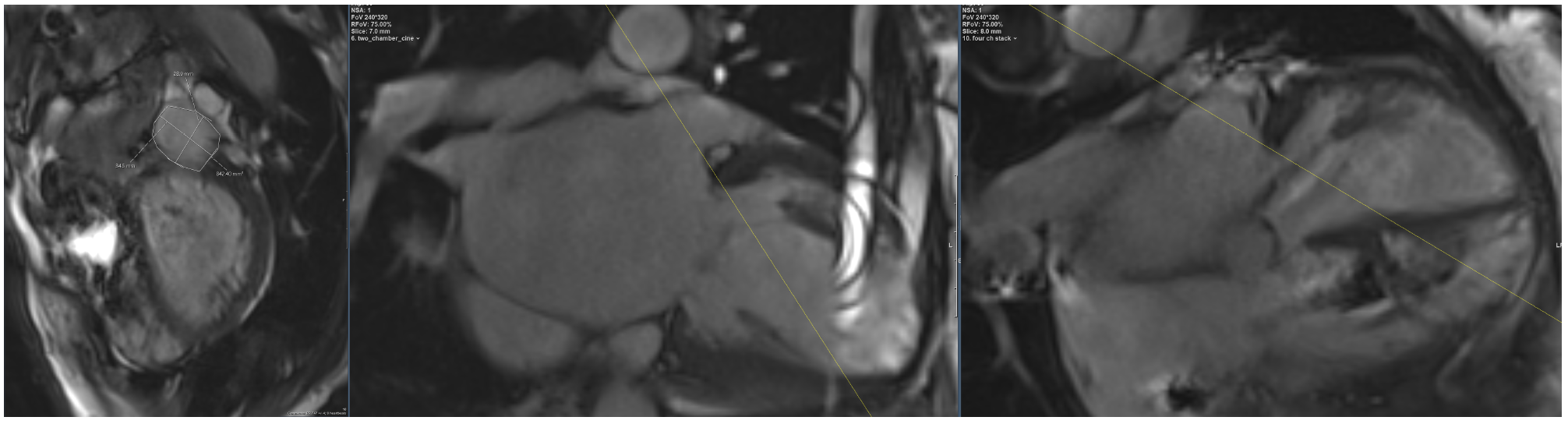
Based on cine imaging, early long-T1 imaging, and late gadolinium imaging did not demonstrate LAA thrombus (Figure 1). The measurements of the LAA ostium were as follows: area 717 mm2, maximum diameter 32 mm, minimum diameter 28 mm and depth 34 mm (Figure2, panel A-C). Based on the left atrial appendage measurements acquired by CMR, a 35 mm WATCHMAN device was selected (1).
Relevant Catheterization Findings
Right common femoral vein access was obtained with micropuncture technique under ultrasound guidance. The Seldinger technique was then performed to place two 8 French Sheaths. The left atrium was accessed using an AcuNav intracardiacechocardiographic (ICE) probe. A Baylis needle was utilized for transeptal puncture and a Double Curve access sheath was used for device deployment. Angiography of the left atrial appendage was performed using a 6 French angled pigtail catheter.
Interventional Management
Procedural Step
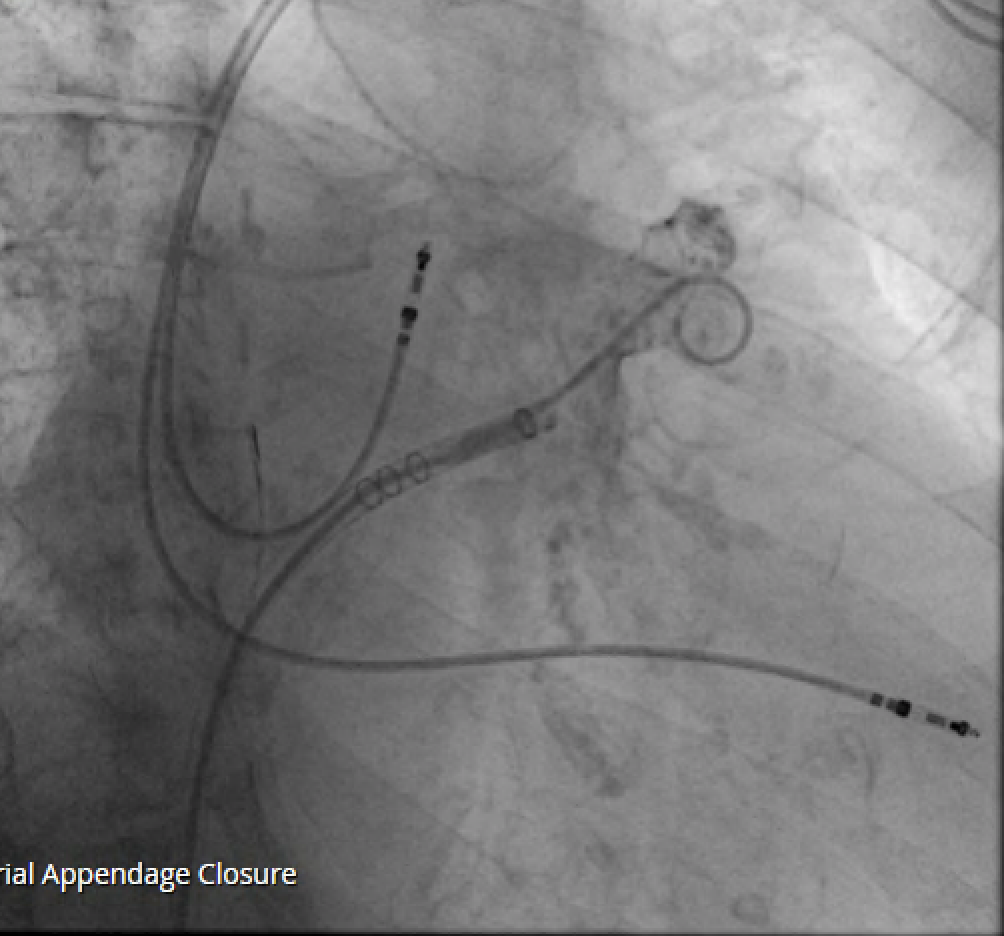
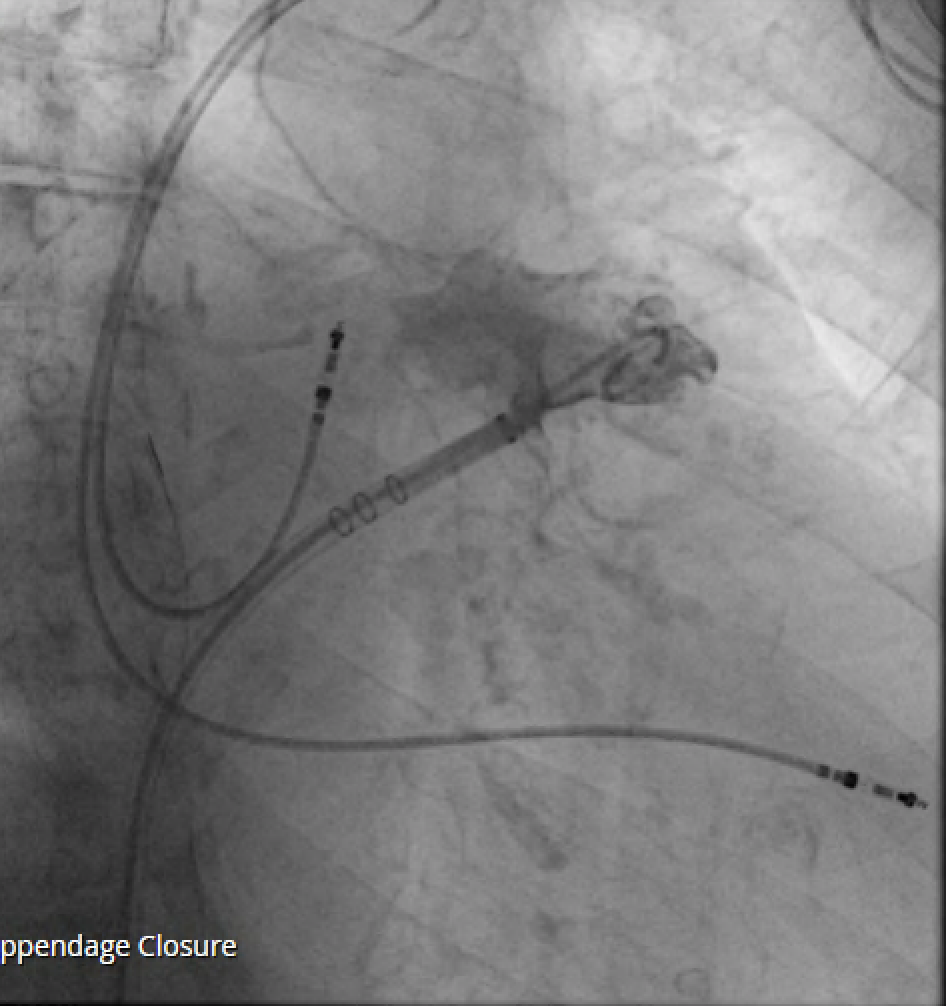
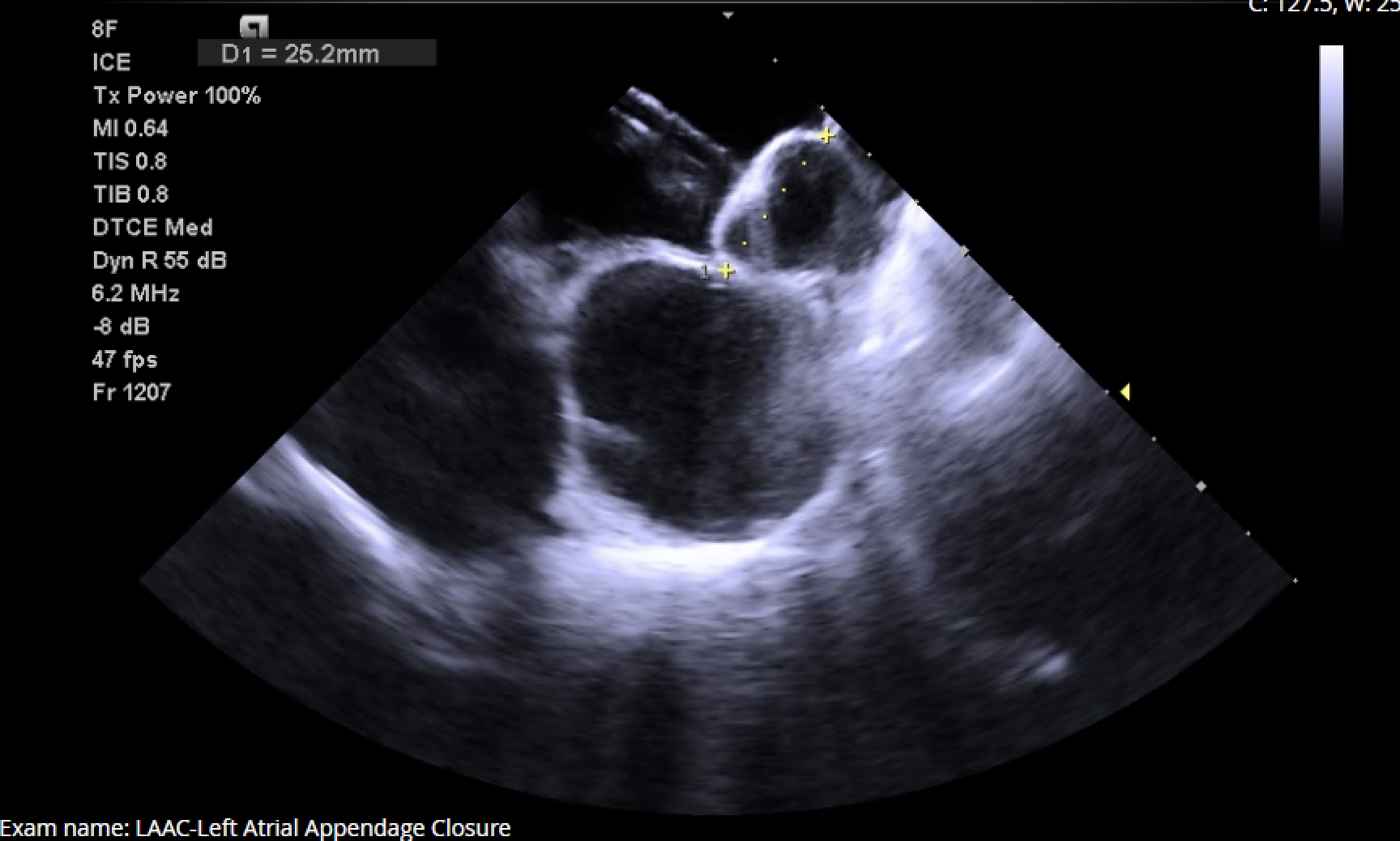
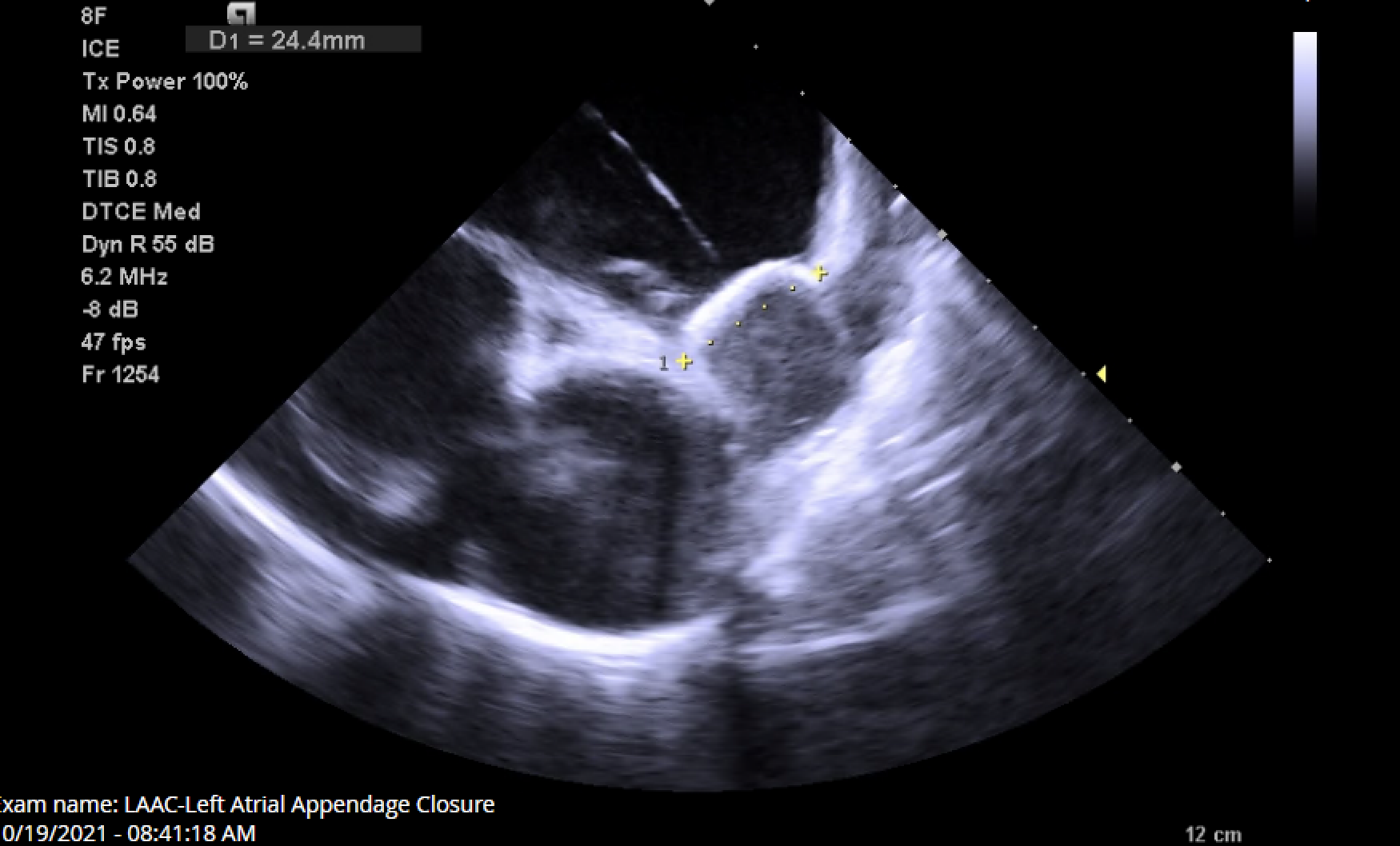
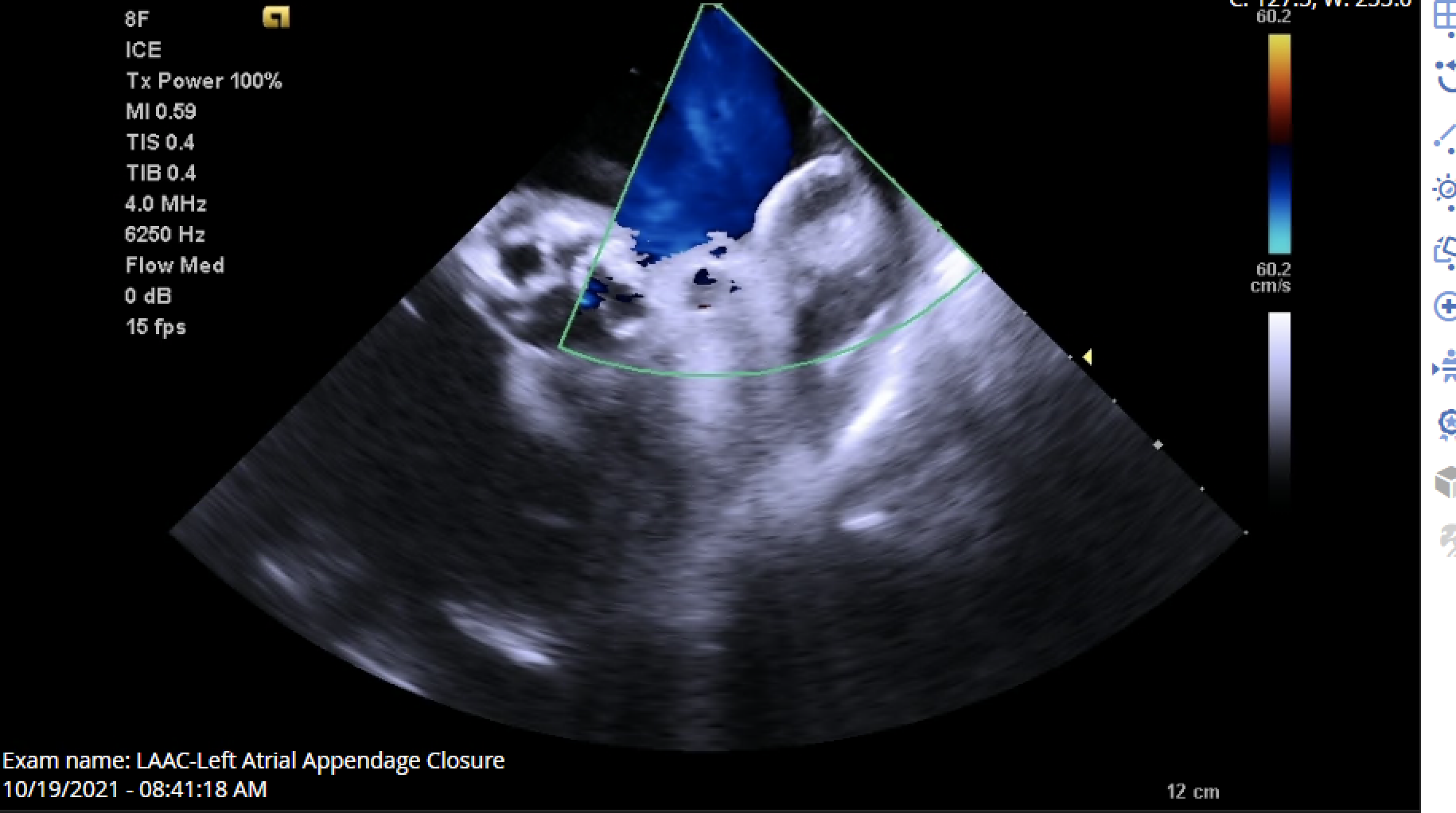
Right common femoral vein access was obtained with micropuncture technique under ultrasound guidance. The Seldinger technique was then performed to place two 8 French Sheaths. Heparin was administered to achieve an appropriate activating clotting time. The left atrium was accessed using an AcuNav intracardiac echocardiographic (ICE) probe. A Baylis needle was utilized for transeptal puncture and a Double Curve access sheath was used for device deployment. Angiography of the left atrial appendage was performed using a 6 French angled pigtail catheter. LAAC device sizing was confirmed via angiography and ICE imaging (Figure 5, panel A-C). After satisfying the P.A.S.S. (Position, Anchor, Size, Seal) criteria, a 35 mm WATCHMAN™ FLX device was successfully deployed with 28% compression. The patient was uneventfully discharged home on the same day.
Case Summary
CTA and TEE are both accepted imaging modalities for LAAC planning2-4. However, TEE used for structural interventions has been associated with serious complications4-5. While CTA has advantages over TEE for LAAC planning, it is contraindicated in patients with renal dysfunction. Our case report highlights the possibility of using CMR for select patients. Here we present a case in which a patient was unable to tolerate TEE from prior stroke and CTA was contraindicated due to renal dysfunction. CMR provided detailed anatomy of the LAA, without risk of renal injury or radiation exposure, and accurately predicted the appropriately-sized device in our patient.
REFERENCES
1. Nadeem F, Igwe C, Stoycos S, Jaswaney R, Tsushima T, Al-Kindi S, Bansal E, Fares A, Dallan L, Patel S, Rajagopalan S, Arruda M, Filby S, Bezerra H. A new WATCHMAN sizing algorithm utilizing cardiac CTA. Cardiovasc Revasc Med. 2021 Jan 12:S1553-8389(21)00012-9. doi: 10.1016/j.carrev.2021.01.009. Epub ahead of print. PMID: 33526392.
2. Möbius-Winkler S, Majunke N, Sandri M, Mangner N, Linke A, Stone GW, Dähnert I, Schuler G, Sick PB. Percutaneous left atrial appendage closure: Technical aspects and prevention of periprocedural complications with the watchman device. World J Cardiol. 2015 Feb 26;7(2):65-75. doi: 10.4330/wjc.v7.i2.65. PMID: 25717354; PMCID: PMC4325303.
3. Galea R, Räber L, Fuerholz M, Häner JD, Siontis GCM, Brugger N, Moschovitis A, Heg D, Fischer U, Meier B, Windecker S, Valgimigli M. Impact of Echocardiographic Guidance on Safety and Efficacy of Left Atrial Appendage Closure: An Observational Study. JACC Cardiovasc Interv. 2021 Aug 23;14(16):1815-1826. doi: 10.1016/j.jcin.2021.05.042. PMID: 34412799.
4. Freitas-Ferraz AB, Rodés-Cabau J, Junquera Vega L, Beaudoin J, O'Connor K, Turgeon PY, Paradis JM, Ferreira-Neto A, Asmarats L, Champagne J, O'Hara G, Bernier M. Transesophageal echocardiography complications associated with interventional cardiology procedures. Am Heart J. 2020 Mar;221:19-28. doi: 10.1016/j.ahj.2019.11.018. Epub 2019 Dec 9. PMID: 31896037.
5. Aragam JR, Almarzooq ZI. Transesophageal Echocardiography in Structural Heart Interventions: Is it Time to Rethink Our Approach? J Am Coll Cardiol. 2020 Jun 30;75(25):3174-3176. doi: 10.1016/j.jacc.2020.05.018. PMID: 32586592