
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-053
A Challenging Right Coronary Artery Chronic Total Occlusion Required Hybrid Approach and Multiple Troubleshooting to Achieve Success
By Hou Tee Lu, Heng Shee Kim, Adelyn Nisha Henry, Chu Zhen Quek, Yu Ying Ong, Azrina Abdul Kadir
Presenter
Hou Tee Lu
Authors
Hou Tee Lu1, Heng Shee Kim1, Adelyn Nisha Henry1, Chu Zhen Quek1, Yu Ying Ong2, Azrina Abdul Kadir3
Affiliation
Sultanah Aminah Hospital, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, KPJ Bandar Dato Onn Specialist Hospital, Malaysia3,
View Study Report
TCTAP C-053
CORONARY - Chronic Total Occlusion
A Challenging Right Coronary Artery Chronic Total Occlusion Required Hybrid Approach and Multiple Troubleshooting to Achieve Success
Hou Tee Lu1, Heng Shee Kim1, Adelyn Nisha Henry1, Chu Zhen Quek1, Yu Ying Ong2, Azrina Abdul Kadir3
Sultanah Aminah Hospital, Malaysia1, Sultan Idris Shah Serdang Hospital, Malaysia2, KPJ Bandar Dato Onn Specialist Hospital, Malaysia3,
Clinical Information
Patient initials or Identifier Number
TFW
Relevant Clinical History and Physical Exam
A 58-year-old man presented with frequent exertional angina for 2 weeks. He was not a smoker or drinker. Sedentary lifestyle. He has medical history of diabetes mellitus and dyslipidemia. He has regular follow ups with his family doctor and he was on Diamicron 80 mg bd, metformin 500 mg bd and atorvastatin 20 mg od. On examination, the hemodynamic was stable. The heart rate was 80/min and blood pressure was 130/80 mmHg. His BMI was 28.
Relevant Test Results Prior to Catheterization
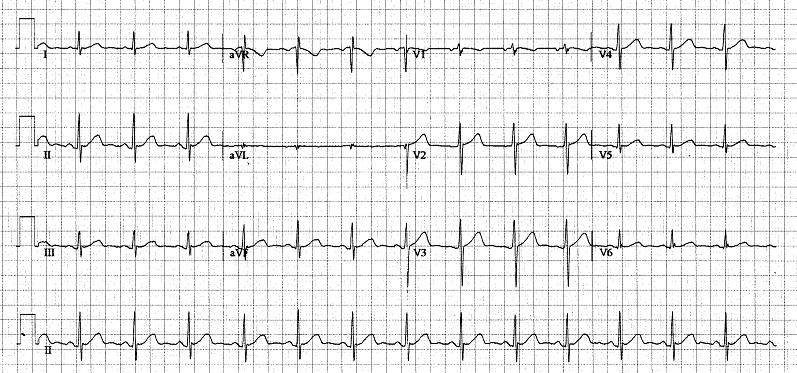
The baseline ECG was normal. The stress test was positive and showed horizontal ST segment depression at II, III, AVF, and V5-6. The blood investigations: Hb: 14.5 g/dL, creatinine: 77 µmol/L, total cholesterol: 5.5 mmol/L, LDL: 2.3 mmol/L, and HbA1C: 8.2%. The echocardiography showed normal EF of 73%. Normal valves and chambers sizes. The CXR was normal.

Relevant Catheterization Findings
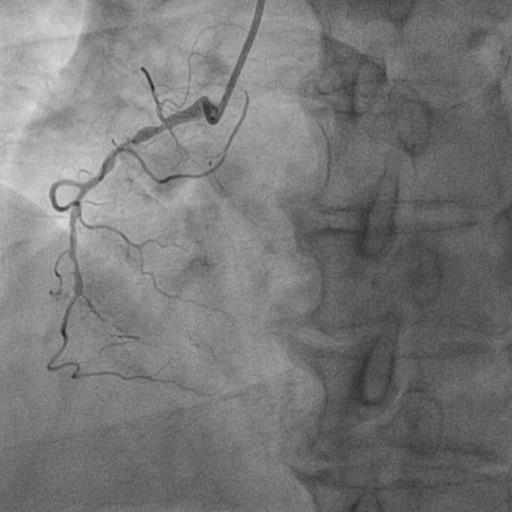
Diagnostic coronary angiogram:1. LMT normal 2. Mid LAD artery 70% stenosis2. Proximal LCX artery 70% stenosis – giving an atrialventricular groove collateral (CC) to rPLV3. Mid RCA 100% stenosis (CTO) J-CTO score: 1 (Clear proximalcap, lesion length > 20mm, non-calcified, non-tortuous, no previous attempt).The SYNTAX score was > 33. Recommended CABG. But patient declined CABG. Proceed for PCI.


Interventional Management
Procedural Step
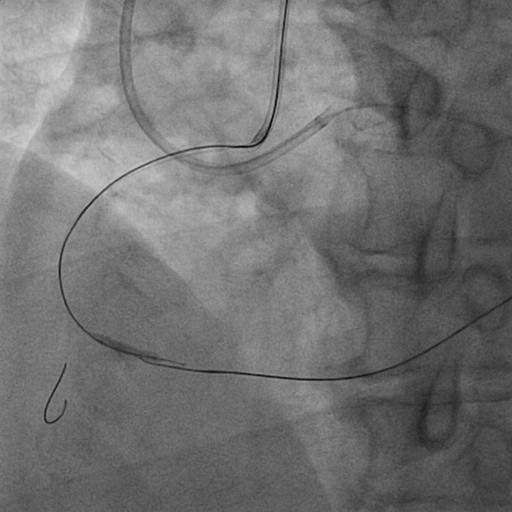
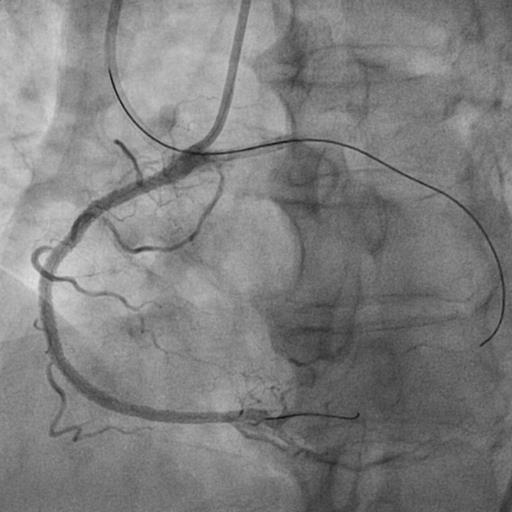
Right and left femoral arteries were punctured. A 7Fr EBU 3.5 was used to engage LMT. JR 4.0 for RCA. Dual injection was performed. Attempted antegrade crossing using a Caravel 135 cm microcatheter (MC) and Fielder XTR guidewire (GW) but was unsuccesful. Wire was escalated to a GAIA 2nd but failed to advance antegradely at mid RCA CTO body. Therefore, retrograde approach was attempted with a Sion wired through AV CC from LCX to rPLV via CARAVEL 150 cm MC. Distal cap was punctured with Fielder XTR, and reverse CART was performed at distal RCA. The retrograde XTR was changed to a Sion wire. The retrograde Sion was managed to be externalized to antegrade guide. However, retrograde MC was unable to cross the distal cap despite multiple attempts. The next attempt was "Tip in" method into externalized retrograde GW (in antegrade guide). Antegrade MC was successfully tipped into retrograde GW. Unfortunately, the antegrade MC also failed to cross CTO body antegradely by tracking along the retrograde GW. After multiple failed attempts to cross antegrade and retrogarde MC through CTO body, decided to leave the retrograde GW into the distal cap as a marker wire and to attempt antegrade crossing. Fortunately, antegrade GAIA 2nd was managed to cross CTO body into PDA. Subsequent balloon angioplasty was done using NC balloons and two EES were implanted with good result and TIMI 3 flow. The LCX and LAD lesions were subsequently treated by a stage procedures.

Case Summary
CTO PCI can be challenging at each and every step. A careful planning, hybrid approach, and awareness of different techniques and tools to overcome challenges and avoid complications are key to success.