
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-051
Szabo Technique for Accurate Stent Placement
By Alvin Tonang, Sodiqur Rifqi
Presenter
Alvin Tonang
Authors
Alvin Tonang1, Sodiqur Rifqi2
Affiliation
Tugurejo Hospital, Semarang, Indonesia1, Dr. Kariadi General Hospital, Indonesia2,
View Study Report
TCTAP C-051
CORONARY - Bifurcation/Left Main Diseases and Intervention
Szabo Technique for Accurate Stent Placement
Alvin Tonang1, Sodiqur Rifqi2
Tugurejo Hospital, Semarang, Indonesia1, Dr. Kariadi General Hospital, Indonesia2,
Clinical Information
Patient initials or Identifier Number
Mr. MAB
Relevant Clinical History and Physical Exam
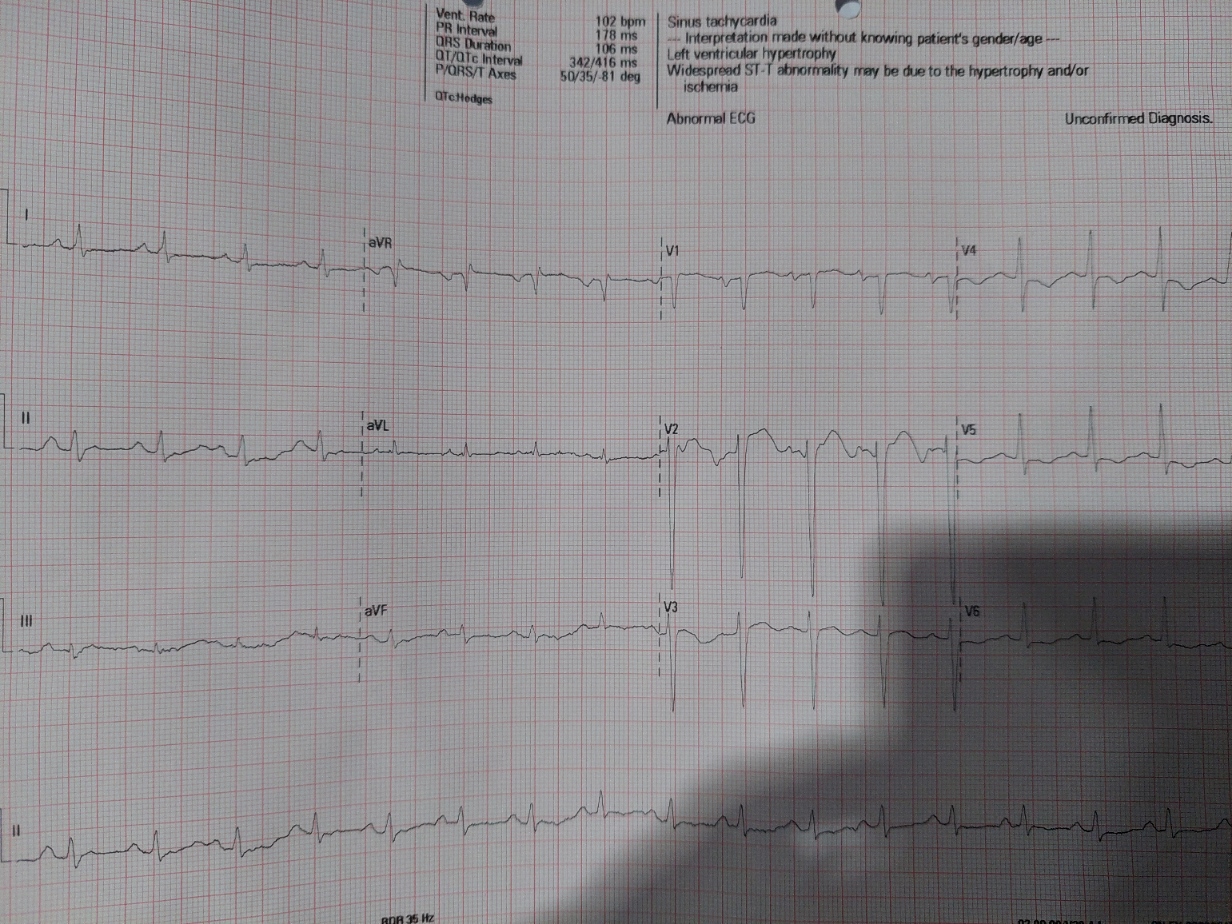
We presented a 37-year-old male hospitalized with heart failure reduced ejection fraction functional class NYHA II-III and smoker. Resting ECG showed sinus tachycardia, with heart rate of 110 bpm and poor R wave progression in anterior lead. Echocardiography showed reduced ejection fraction of 21% with extensive regional wall motion abnormality. He was treated with heart failure treatment and sent to undergo coronary angiogram for further investigation.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
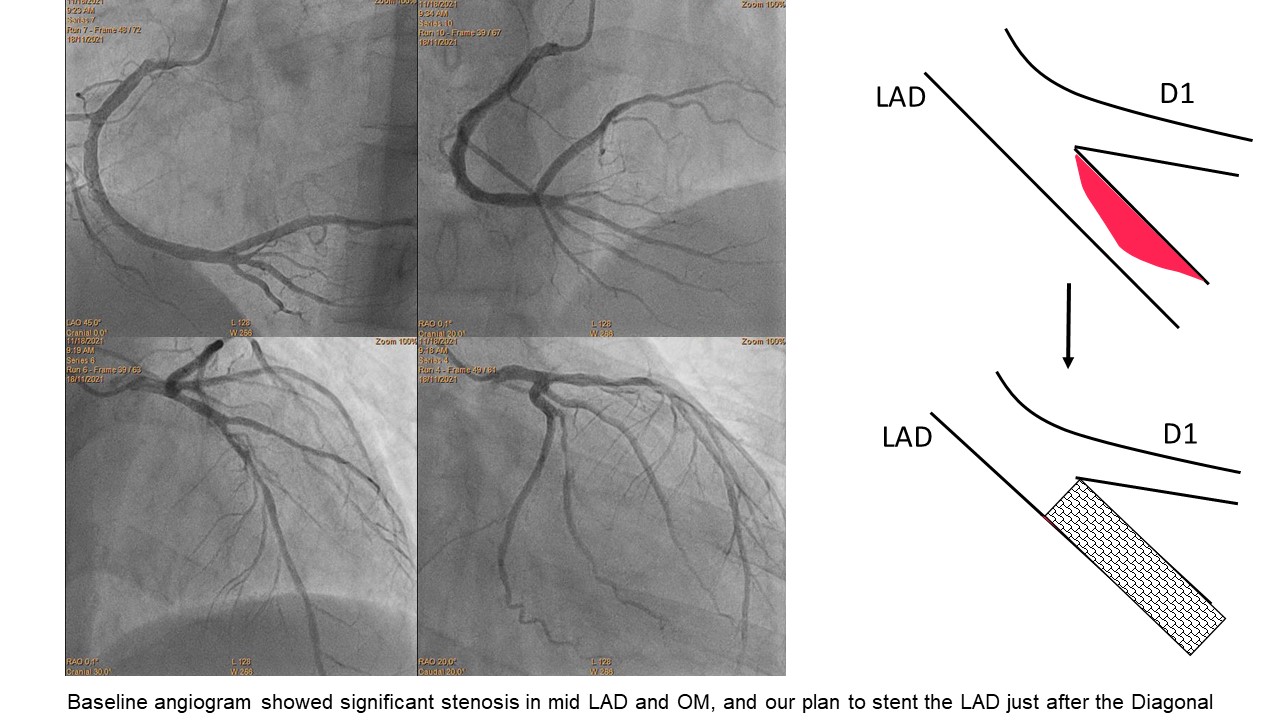
Using right radial approach with 6-F sheath, we did coronary angiography using 5-F Tiger catheter. RCA was dominant and normal. We observed significant stenosis in the mid LAD right after the D1 branch (Medina 0-1-0), and significant stenosis in the proximal OM branch (figure 1). We decided to implant the stent just after the diagonal branch. Reducing the possibility of geographical miss and extensive protrusion, we decided to do Szabo Technique.
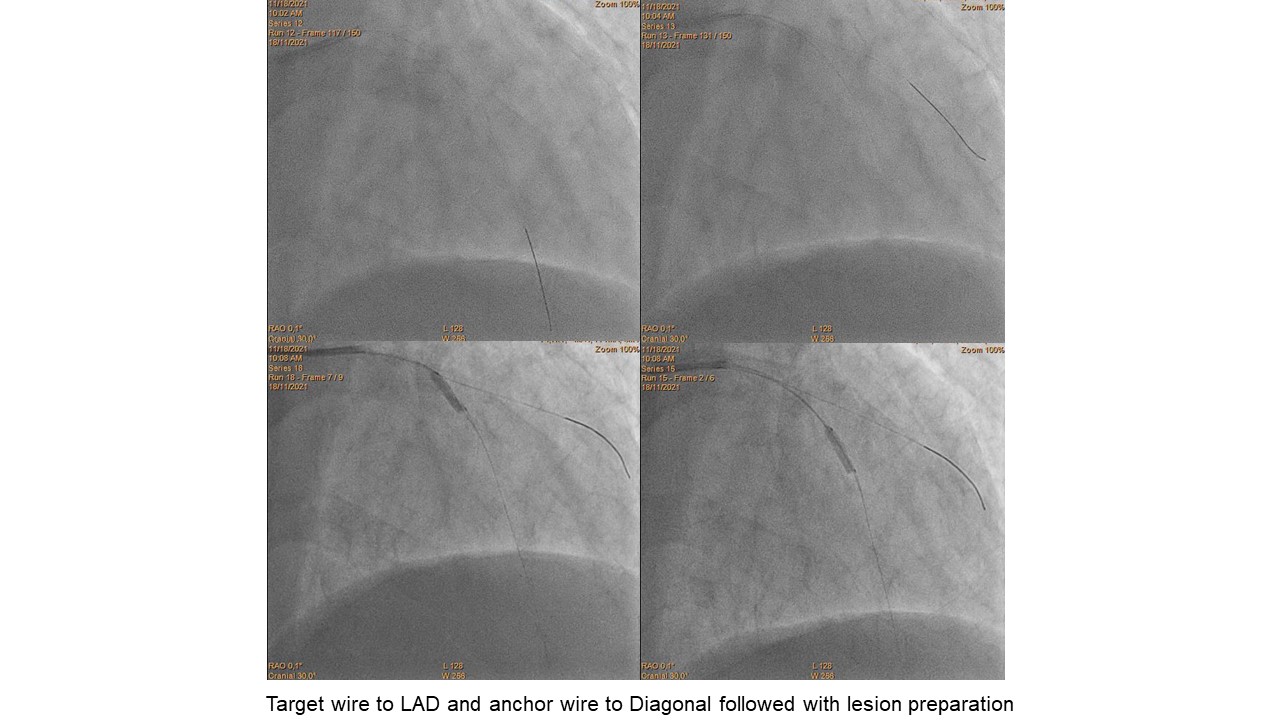
We did PCI using CLS 3,5/6F guide catheter. Successfully wired the LAD using Runthrough guidewire as a target wire, with double wire to the first diagonal branch using Sion Blue as the anchor wire. Predilatation in the mid LAD using scoring balloon 2.5x15 mm (until 12 atm). (figure 2)
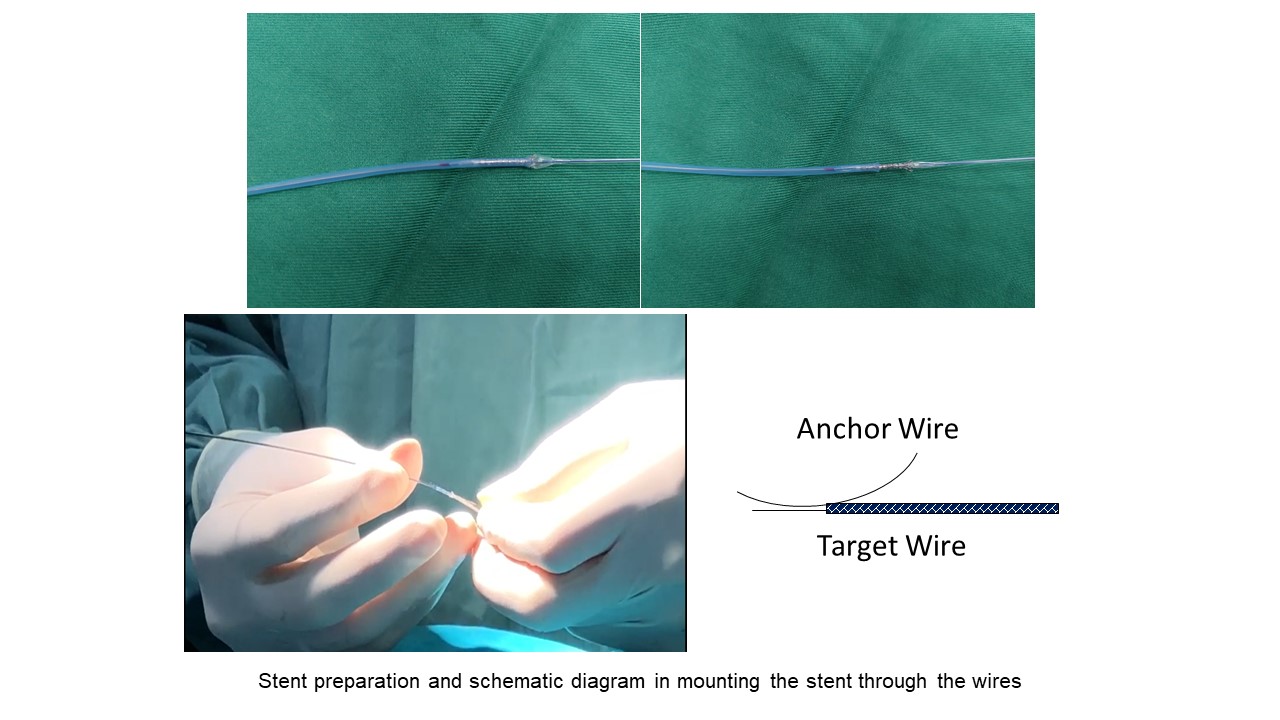
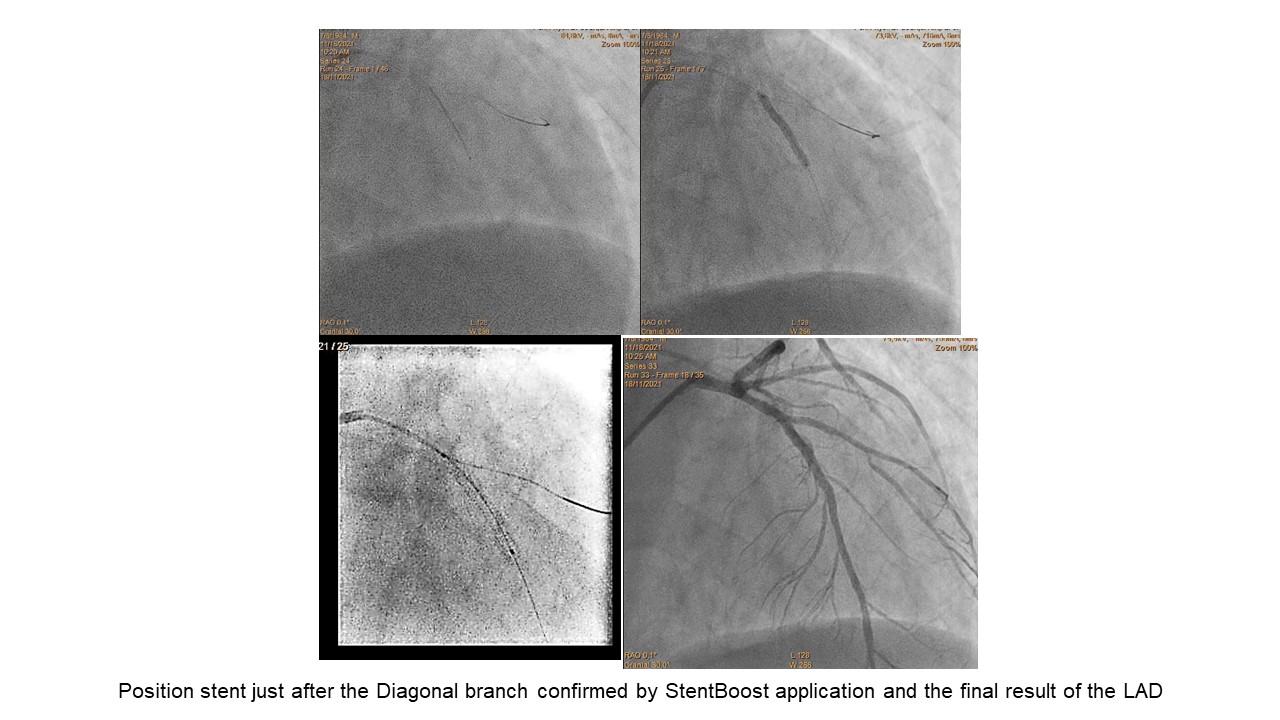
We prepared the DES 2.75x28 mm stent by uncovering the proximal strut and inflating it until 4 atm (figure3). Carefully crimped back the proximal to mid part of the stent and then delivered the stent through the LAD wire. Thus, we mounted the proximal strut with the diagonal wire, and carefully delivered stent through the guiding catheter. Remember to not push excessively against resistance since it can cause stent dislodgement. After positioning the stent right after diagonal branch, we inflated it until 17 atm. The final result showed no residual stenosis and no side branch compromise with TIMI III flow (figure 4).
At follow-up, we observed significant clinical improvement was achieved a week after the procedure.
We did PCI using CLS 3,5/6F guide catheter. Successfully wired the LAD using Runthrough guidewire as a target wire, with double wire to the first diagonal branch using Sion Blue as the anchor wire. Predilatation in the mid LAD using scoring balloon 2.5x15 mm (until 12 atm). (figure 2)
We prepared the DES 2.75x28 mm stent by uncovering the proximal strut and inflating it until 4 atm (figure3). Carefully crimped back the proximal to mid part of the stent and then delivered the stent through the LAD wire. Thus, we mounted the proximal strut with the diagonal wire, and carefully delivered stent through the guiding catheter. Remember to not push excessively against resistance since it can cause stent dislodgement. After positioning the stent right after diagonal branch, we inflated it until 17 atm. The final result showed no residual stenosis and no side branch compromise with TIMI III flow (figure 4).
At follow-up, we observed significant clinical improvement was achieved a week after the procedure.
Case Summary
gBifurcation lesion is one of the challenges in PCI. Obtaining the best stent position with no geographical miss and no extensive protrusion is very important in our case. Originally, Szabo et al. (2015) described a technique where the “stop wire” across the last strut of the stent will facilitate holding the proximal part of the stent right at the exact ostium of the vessel allowing an accurate coverage without excessive stent protrusion in aorto-ostial lesion. Since the publication, there were modifications of the technique and used in intracoronary ostial lesion. In our case, the use of Szabo technique can help us to facilitate accurate stent placement in an efficient and simple way.