
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-043
Left Main Trifurcation Stenting
By Ilfir Mustafin, Igor Dmitriev, Irina E Nikolaeva
Presenter
Igor Dmitriev
Authors
Ilfir Mustafin1, Igor Dmitriev1, Irina E Nikolaeva1
Affiliation
Republican Cardiology Center, Russian Federation1,
View Study Report
TCTAP C-043
CORONARY - Bifurcation/Left Main Diseases and Intervention
Left Main Trifurcation Stenting
Ilfir Mustafin1, Igor Dmitriev1, Irina E Nikolaeva1
Republican Cardiology Center, Russian Federation1,
Clinical Information
Patient initials or Identifier Number
A.A.
Relevant Clinical History and Physical Exam
Patient A.A. who is 66-years-old was hospitalized as planned with complaints of chest pain during exercise (stable angina) pass with the help of taking nitroglycerin, dyspnea. Increased blood pressure to 190/100 mmHg over the years. Deterioration in health for several months.Diagnosis: CHD. Stable angina stage III. Heart failure I st. Left ventricle chronic aneurysm. Hypertension stage 3, 1 degree, risk 4.
Relevant Test Results Prior to Catheterization
ECG - sinus rhythm, heart rate 58 beats per minute, scar changes along the lower wall of the LV.TTE - EF 42%, drop of local LV contractility, hardening of the aorta.Holter monitoring - within normal limits.
Relevant Catheterization Findings
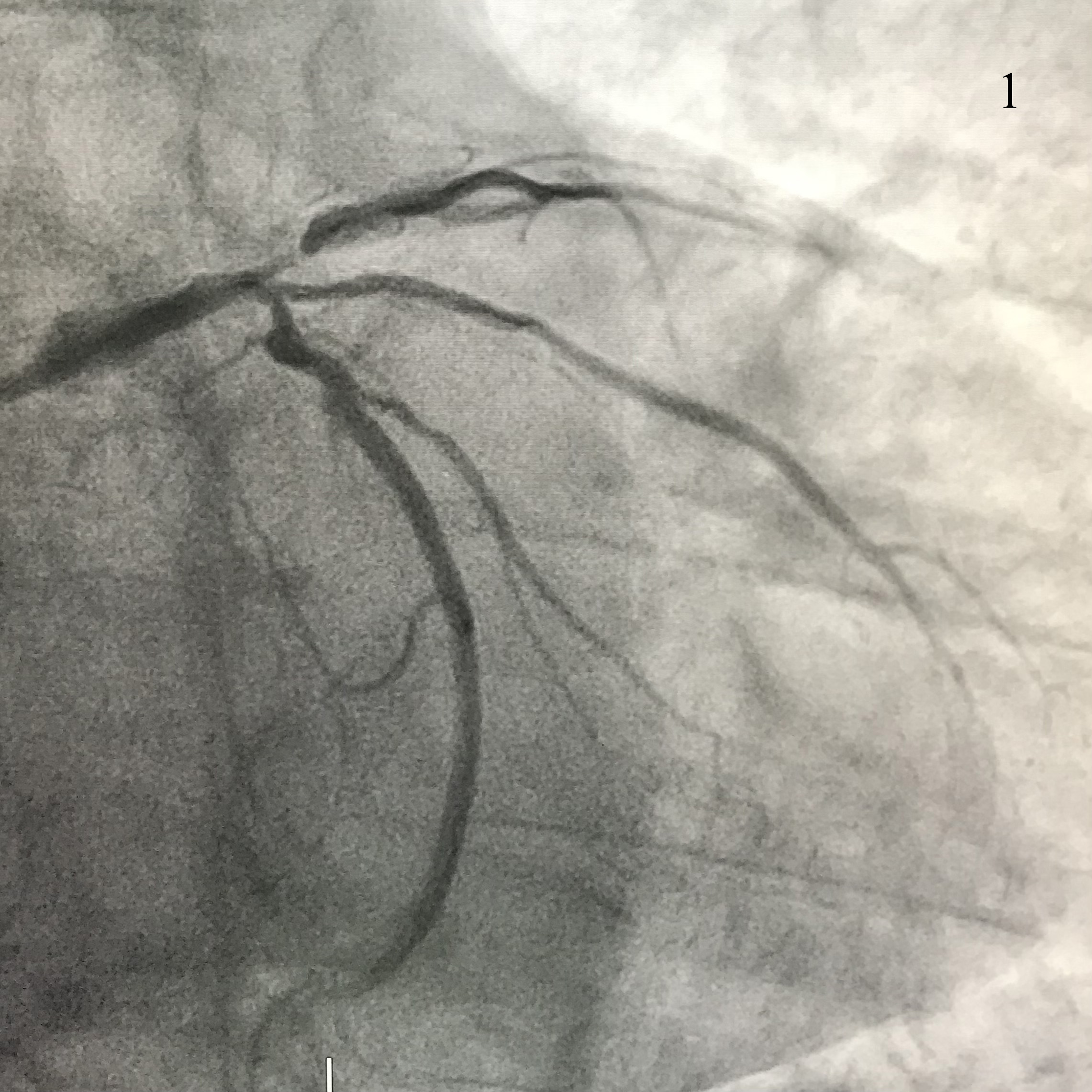
We performed coronary angiography, where a trifurcation lesion LM was found: LM - 75%; LAD - 90%; RI - 80%; LCx - 75-80% (pic. 1).A consultation of the cardiac team was held where it was decided to perform CABG, but the patient refused the operation.
Interventional Management
Procedural Step
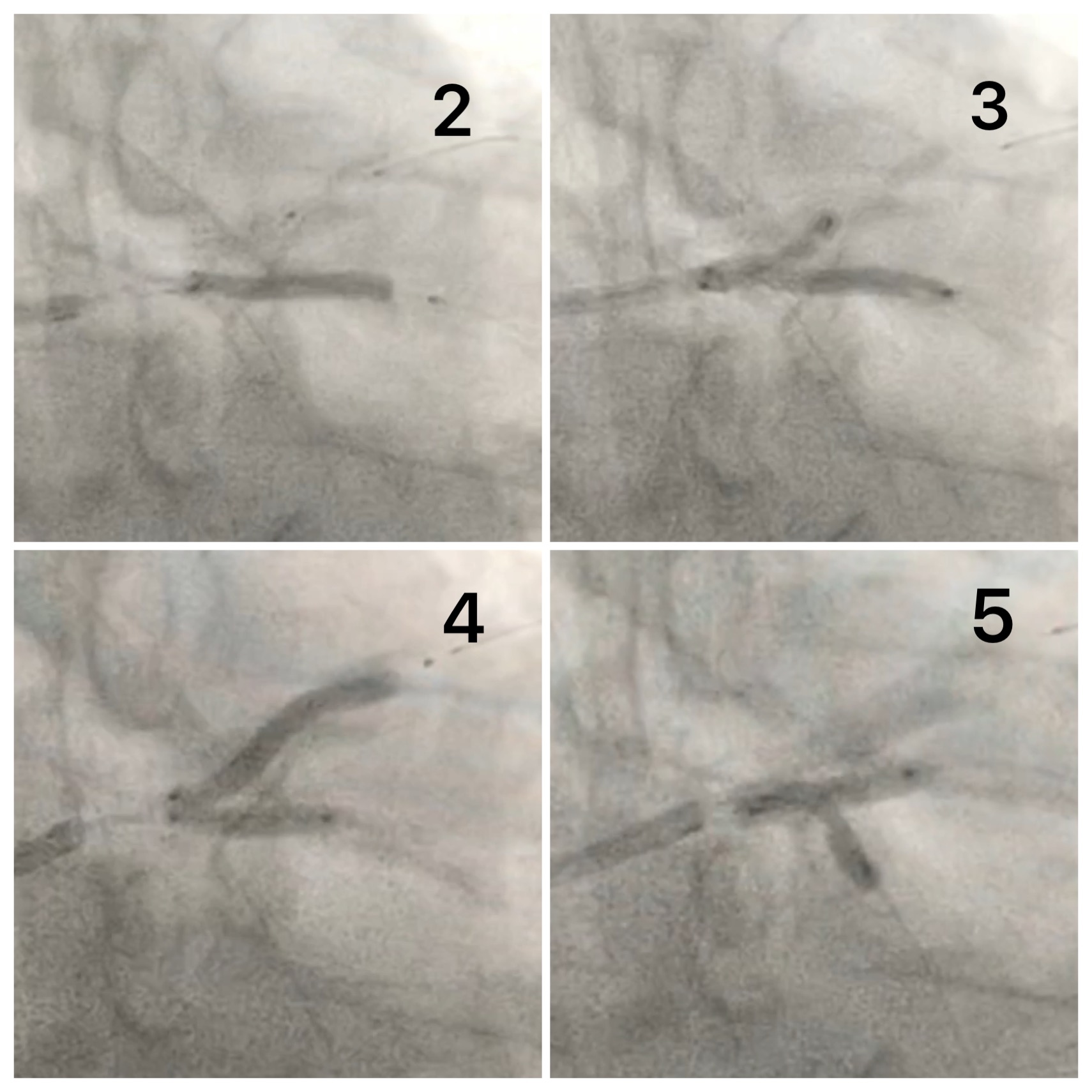
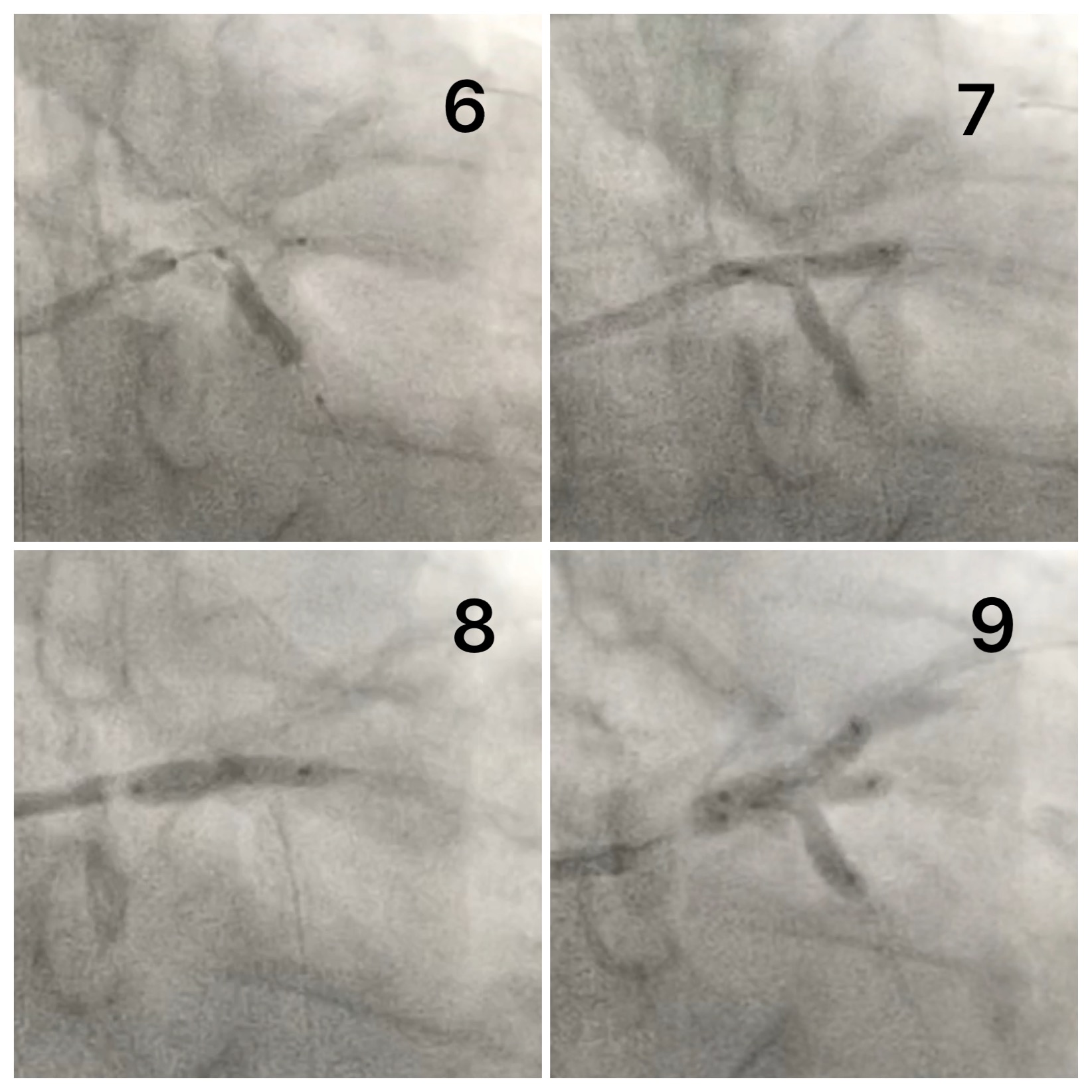
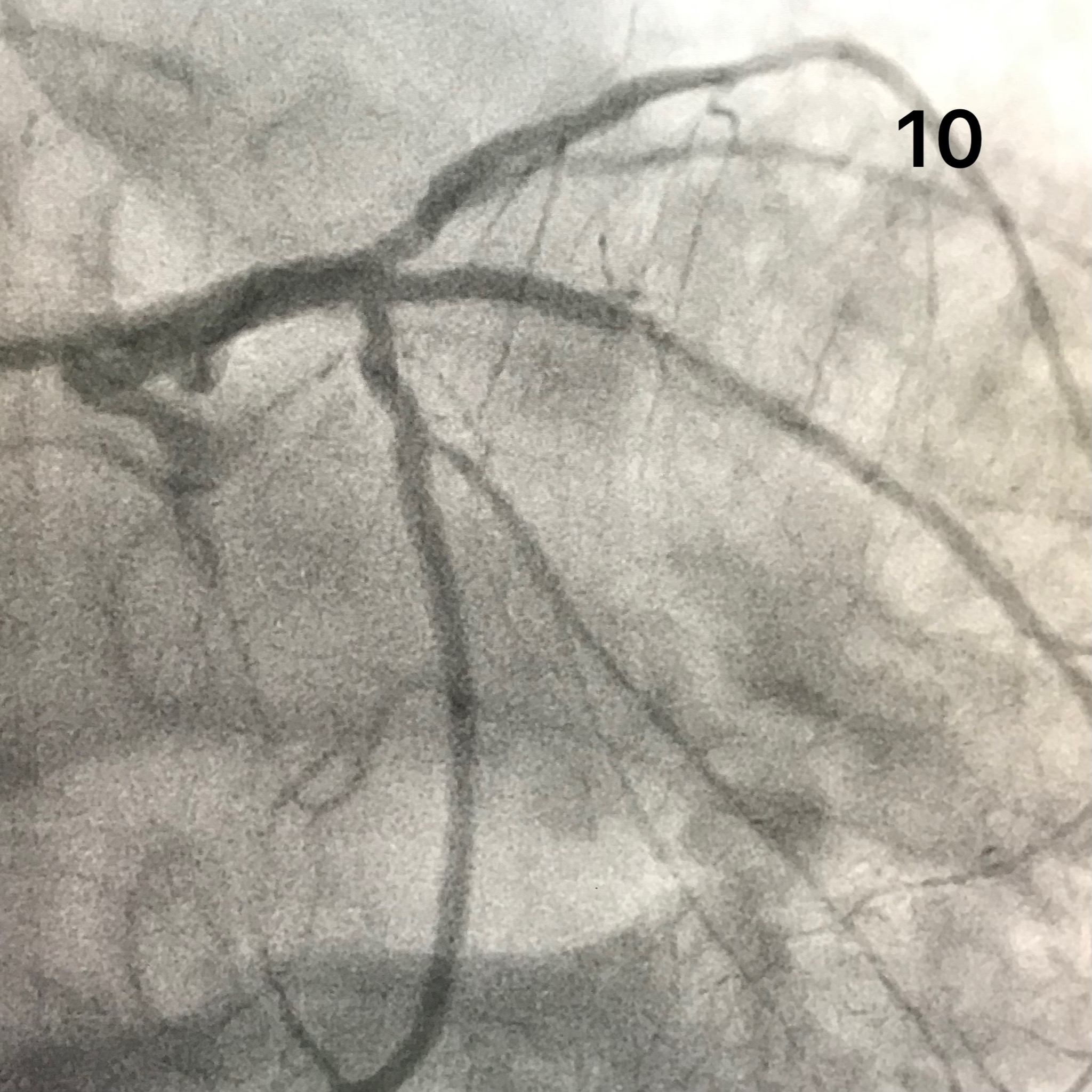
Performed puncture of the radial artery of the 7Fr introducer, lowered three coronary wires in the LAD, RI and LCx.Along the wires, the balloon is 2.5x15 mm in the LAD, and the stent is 2.5x22 mm in the RI. A stent was implanted from the orifice of the RI into the proximal third with a slight protrusion of the distal edge into the LM (pic 2). Performed kissing dilatation with pre-limitation of LAD (Pic. 3).A 2.75x28 mm stent is brought down along the wire in the LAD, and a 2.5x15 mm balloon in the RI. A stent was implanted from the LAD with a small outlet into the LM. Kissing dilation was performed (pic. 4).Recrossing of wires in LCx and RI, followed by kissing dilatation with 2.5x15 mm and 2.5x15 mm balloons (pic 5).Along the wires, the balloon is 2.5x15 mm in the RI, and the stent is 2.5x18 mm in the LCx. The stent was implanted from the ostium of the LCx (pic 6). Performed kissing dilatation with RI and LCx (pic 7).A 4.0x15 mm stent was implanted from the LCA trunk into the RI with low pressure (pic 8).Recrossing of all wires was performed, followed by triple-kissing with 2.5x15 mm (x3) balloons under high pressure (pic 9).Control angiography shows a tight fit of the stents, without signs of dissection and obstruction to blood flow (pic. 10).
Case Summary
On the PubMed website, for similar requests for trifurcation stenting (left main triple stenting, trifurcation stenting, trifurcation ballon, triple kiss, left main trifurcation, etc.), an insufficient number of articles on this topic can be noted and, thus, there is not enough information about the correct technique for performing trifurcation stenting.In this case, the RI diameter allowed us to implant a stent from the LCA trunk into the RI, which, in our opinion, is the best choice for the subsequent triple-kissing technique, since the cells expand from different sides.The method of trifurcation stenting clearly requires long-term result.