
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-073
ECMO Assisted CHIP PCI for a Patient With Single Surviving Vessel With Moderate to Severe Calcified Disease With Severe Biventricular Dysfunction
By Nagendra Boopathy Senguttuvan, Harsimran Singh, Santhosh Kumar Periyasamy, Ramesh Sankaran, Vinod Kumar Balakrishnan, S Sadhanandham, Venkata Balasubramaniyan Jayanty, Preetam Krishnamurthy, Manokar Panchanatham, Thoddi Ramamurthy Muralidharan
Presenter
Nagendra Boopathy Senguttuvan
Authors
Nagendra Boopathy Senguttuvan1, Harsimran Singh2, Santhosh Kumar Periyasamy3, Ramesh Sankaran1, Vinod Kumar Balakrishnan1, S Sadhanandham1, Venkata Balasubramaniyan Jayanty1, Preetam Krishnamurthy1, Manokar Panchanatham1, Thoddi Ramamurthy Muralidharan1
Affiliation
Sri Ramachandra Institute of Higher Education and Research, India1, Pancham Hospital, India2, Sri Ramachandra Medical Center, India3,
View Study Report
TCTAP C-073
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
ECMO Assisted CHIP PCI for a Patient With Single Surviving Vessel With Moderate to Severe Calcified Disease With Severe Biventricular Dysfunction
Nagendra Boopathy Senguttuvan1, Harsimran Singh2, Santhosh Kumar Periyasamy3, Ramesh Sankaran1, Vinod Kumar Balakrishnan1, S Sadhanandham1, Venkata Balasubramaniyan Jayanty1, Preetam Krishnamurthy1, Manokar Panchanatham1, Thoddi Ramamurthy Muralidharan1
Sri Ramachandra Institute of Higher Education and Research, India1, Pancham Hospital, India2, Sri Ramachandra Medical Center, India3,
Clinical Information
Patient initials or Identifier Number
2784128
Relevant Clinical History and Physical Exam
44-year-old female admitted with h/o breathlessness (NYHA III/IV) associated with abdominal distension.BP- 100/60 mmHg, PR- 100/minCVS- S1S2+, no murmurRS- B/L basal crepts +
PAST H/O :-• Old inferior wall MI (DECEMBER 2020)• S/P lysis with reteplase
PAST H/O :-• Old inferior wall MI (DECEMBER 2020)• S/P lysis with reteplase
Relevant Test Results Prior to Catheterization
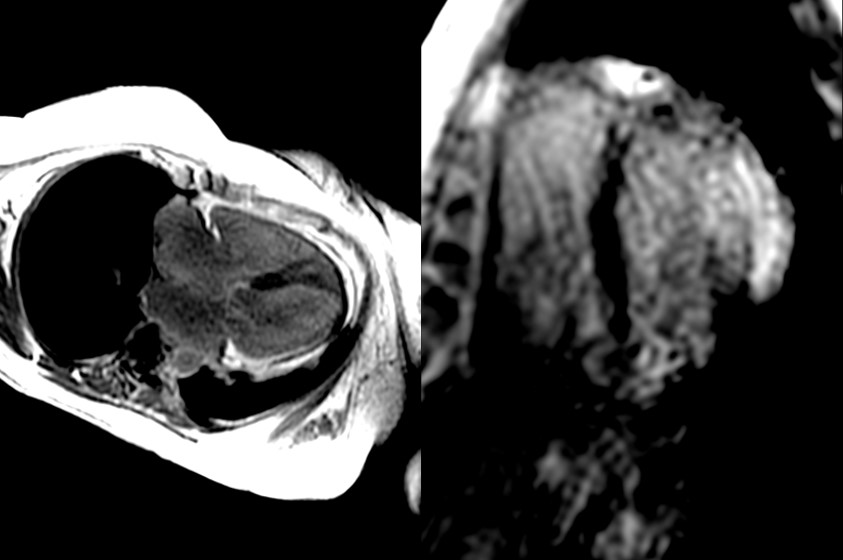
2D TTE- Mildly dilated LV, bicuspid aortic valve, moderate TR with severe PAH (EPAP 72mmHg). Entire inferolateral and inferior wall, basal and mid anterolateral wall thinned and akinetic, apical anterior wall hypokinetic. Moderate to severe LV systolic dysfunction with grade III diastolic dysfunction (EF 32%). Moderate RV dysfunction (TAPSE 1.4cm).
ECG- NSR, no ST-T changes
C-MRI VIABLE LAD TERRITORY. MOST SEGMENTS OF RCA AND LCX ARE NOT VIABLE.
Hb- 9.6 gm/dl
Creatinine- 0.9 mg/dl
 Media28.mp4
Media28.mp4
ECG- NSR, no ST-T changes
C-MRI VIABLE LAD TERRITORY. MOST SEGMENTS OF RCA AND LCX ARE NOT VIABLE.
Hb- 9.6 gm/dl
Creatinine- 0.9 mg/dl
Relevant Catheterization Findings
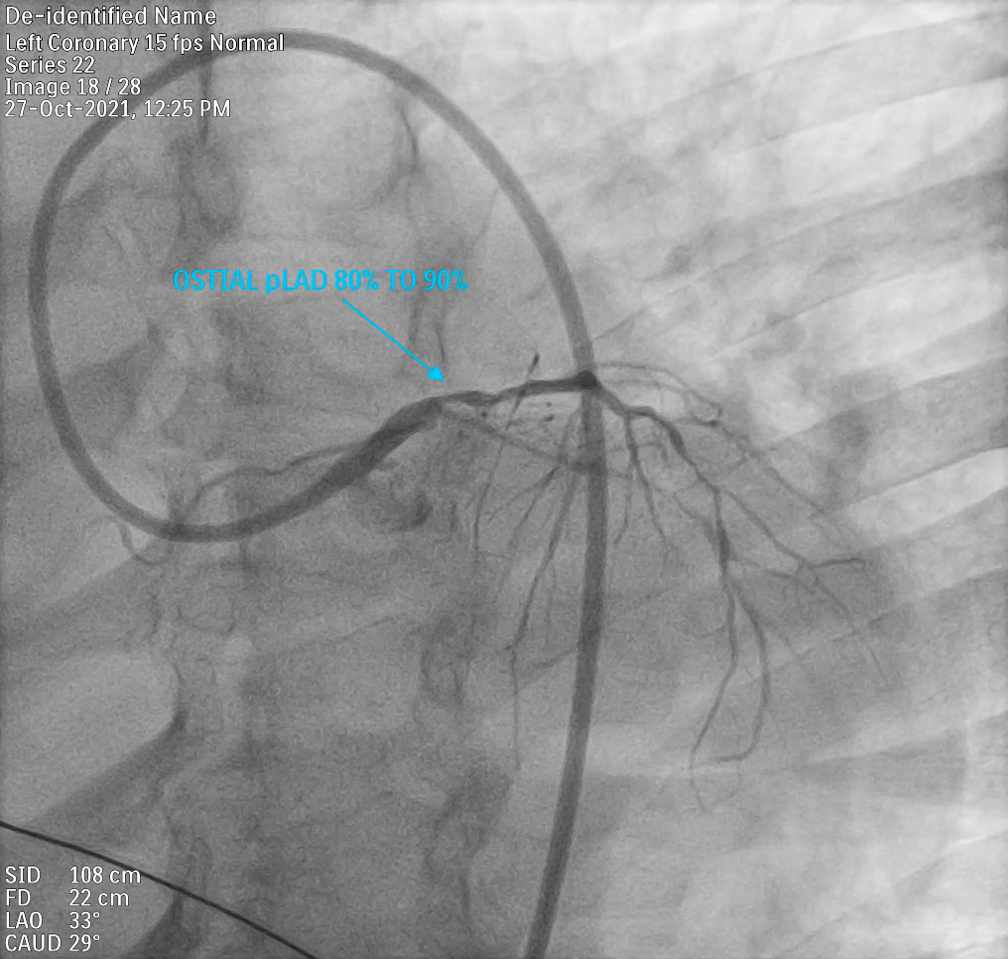
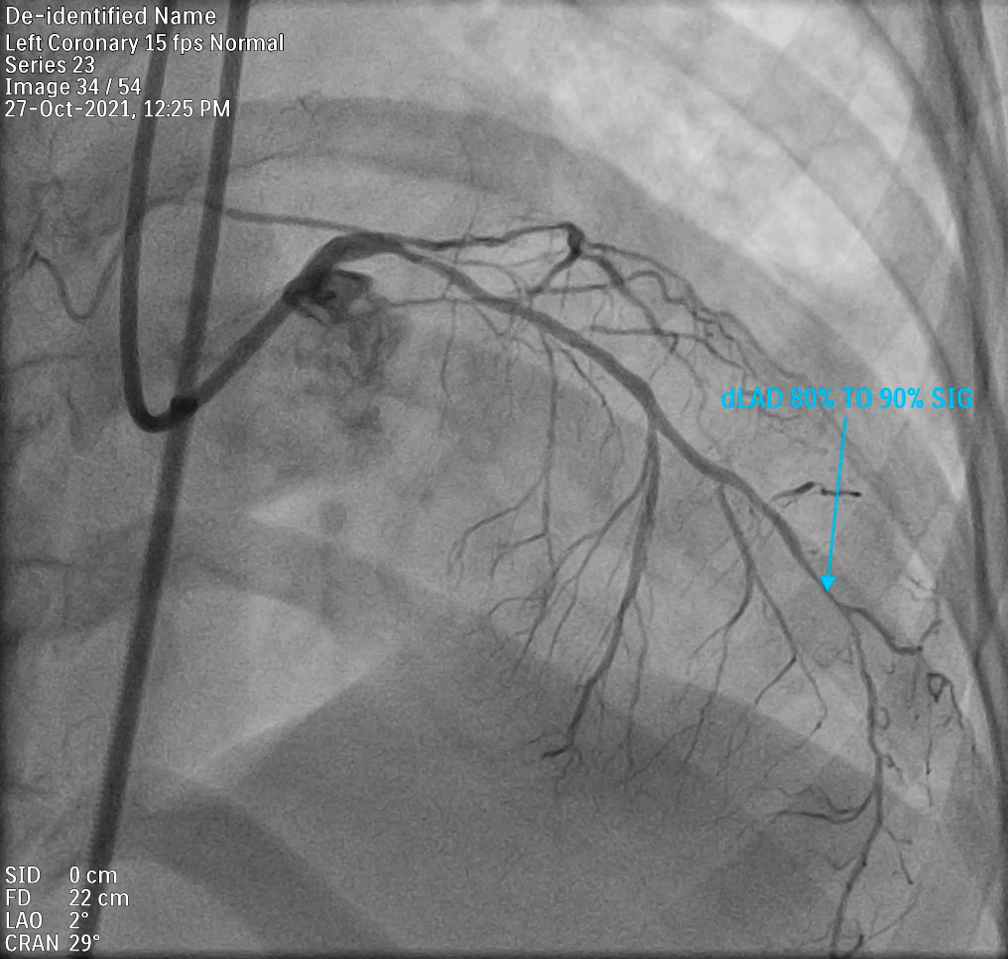
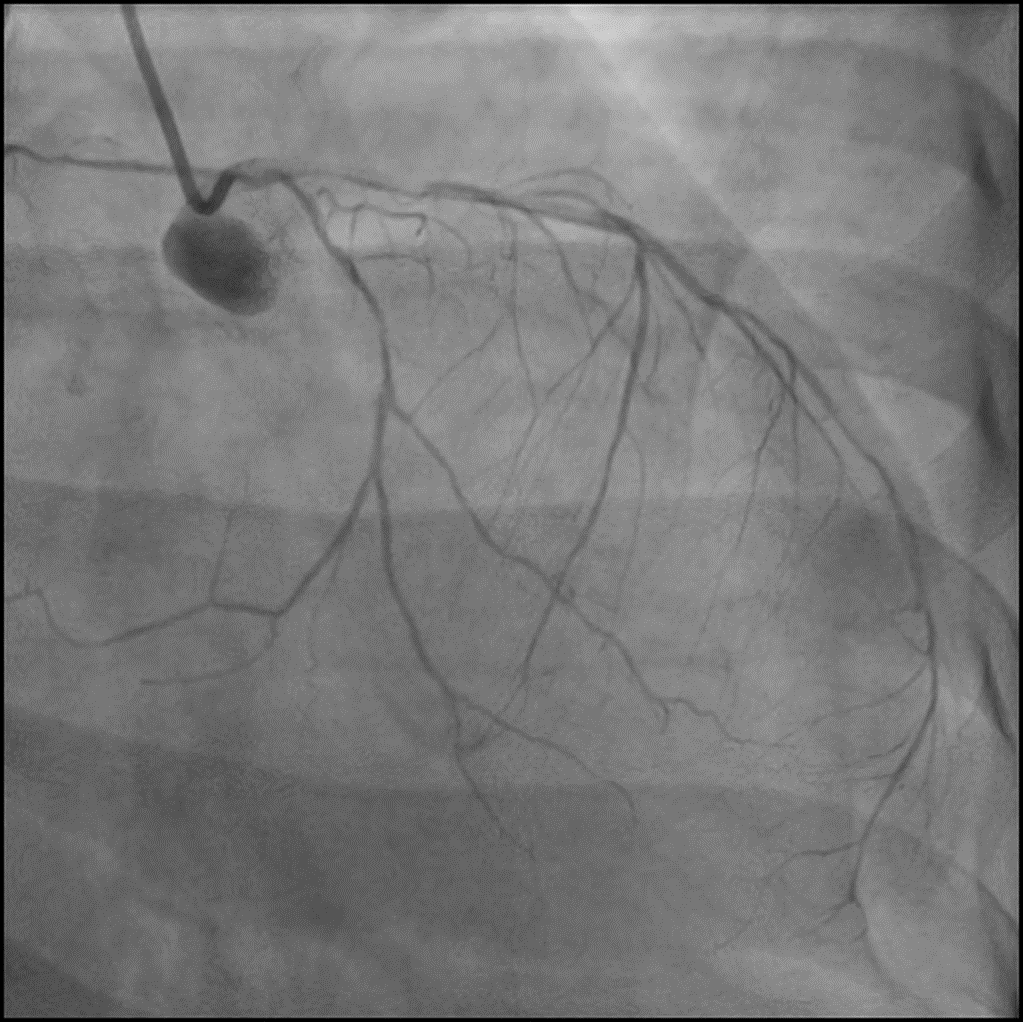
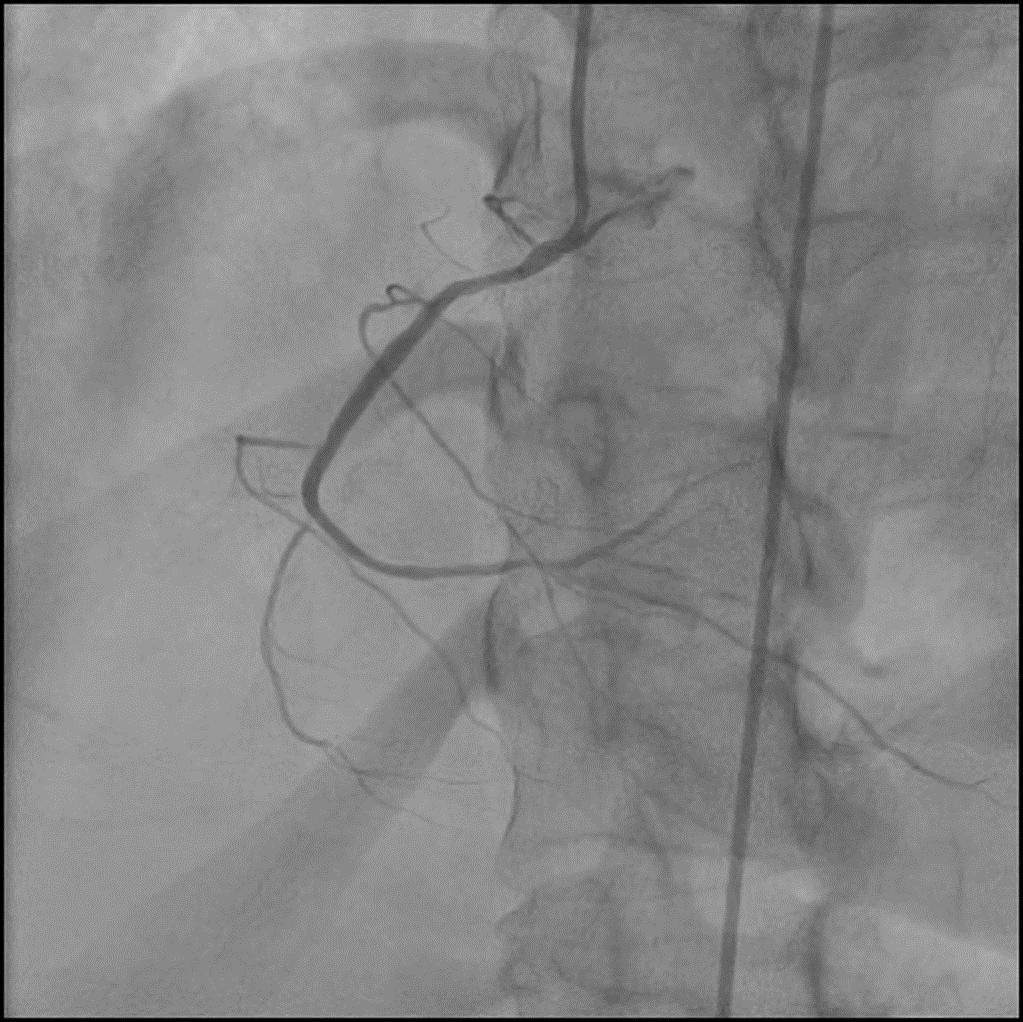
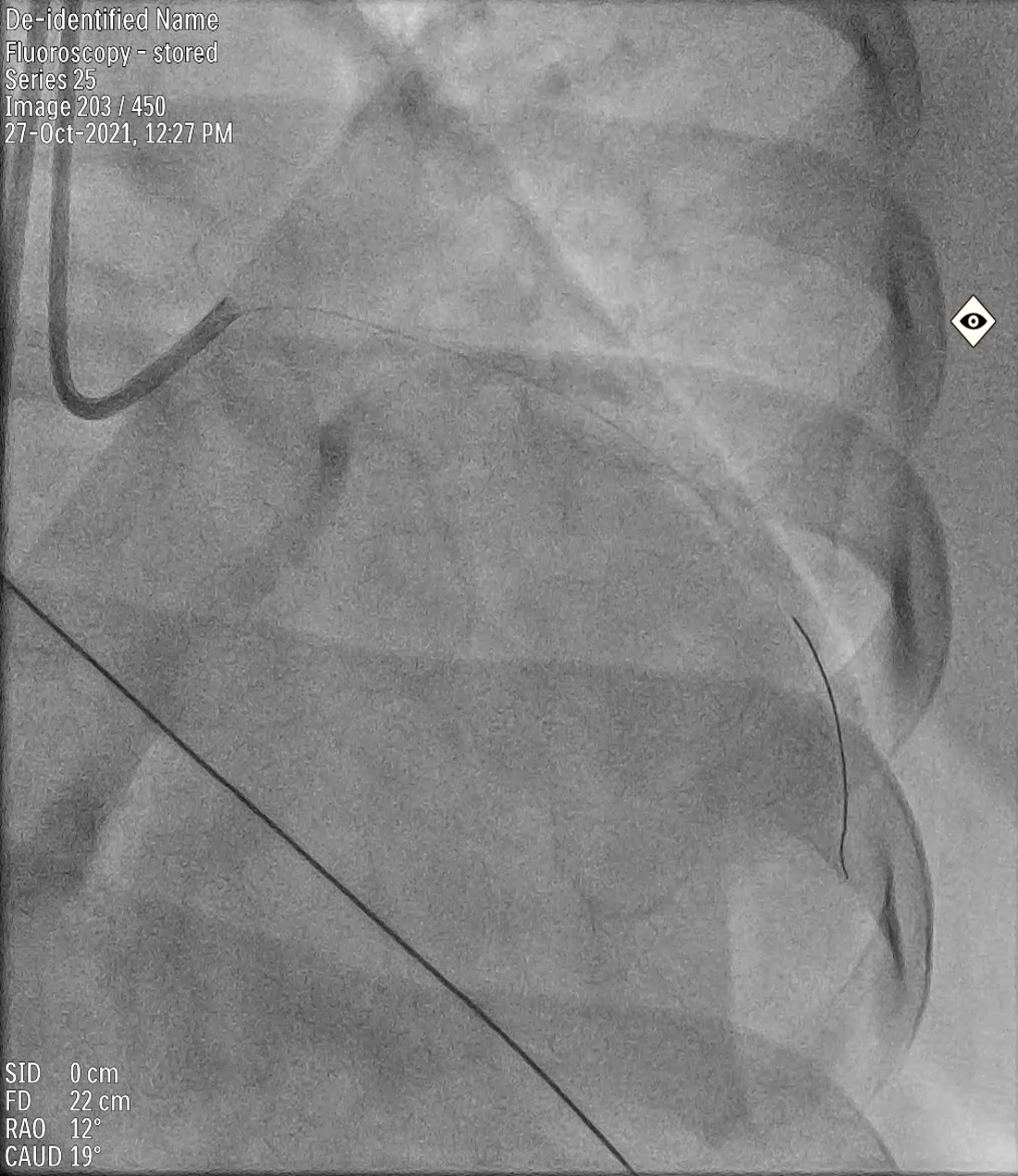
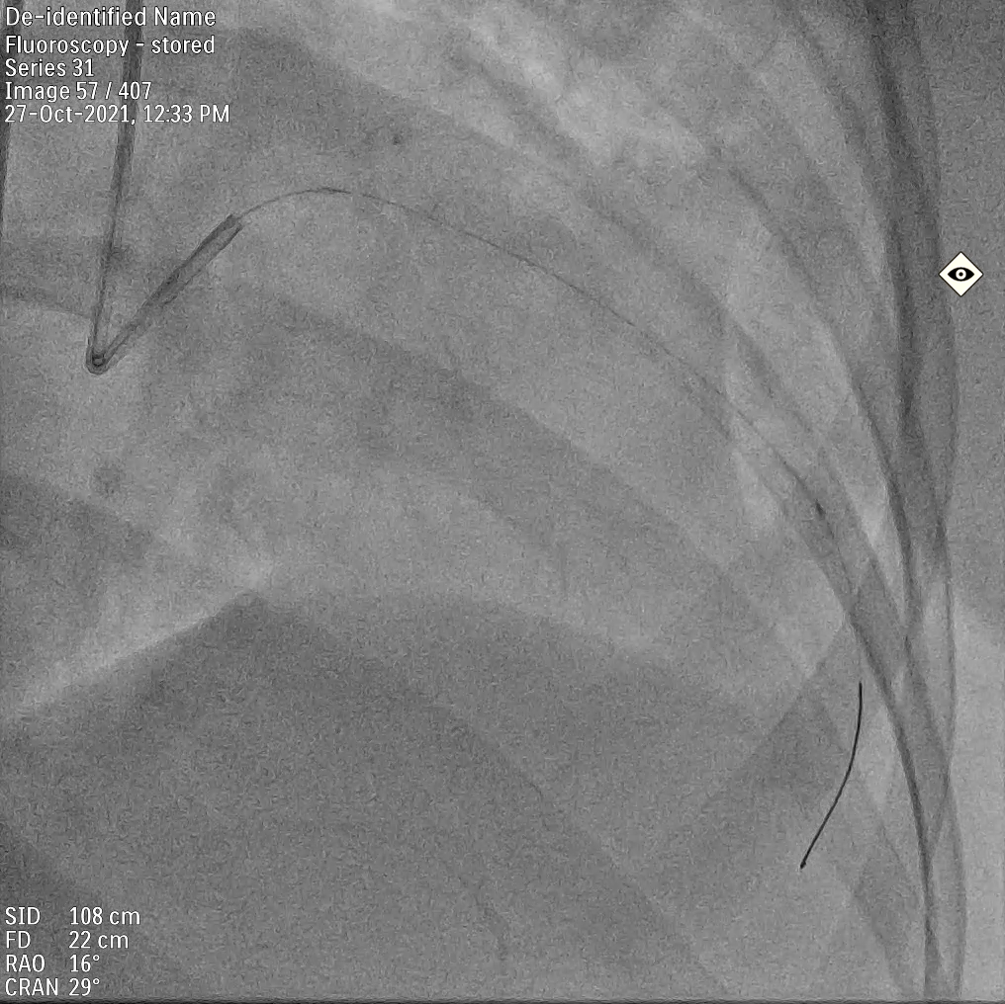
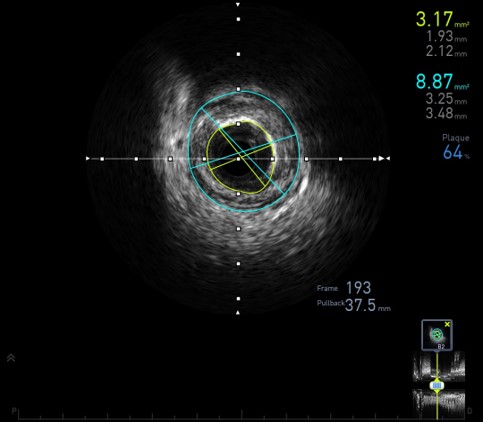
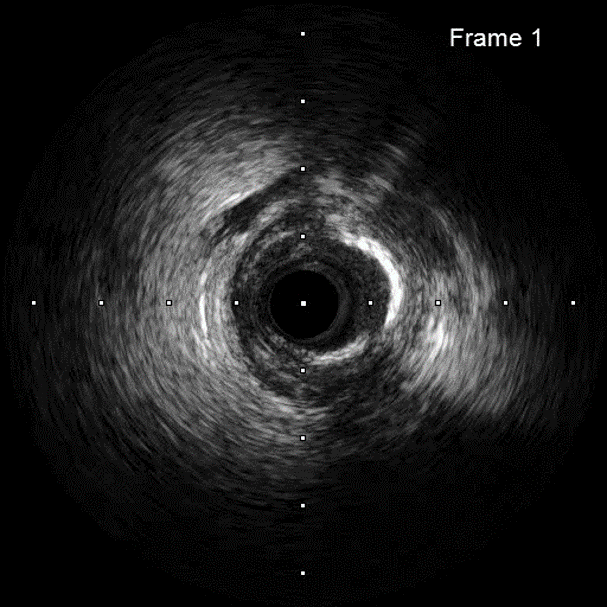
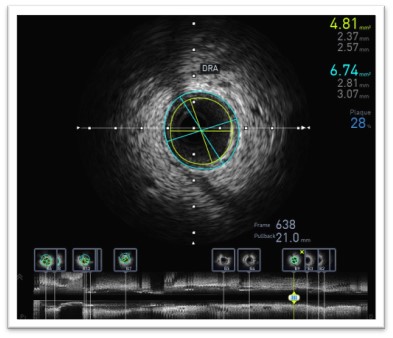
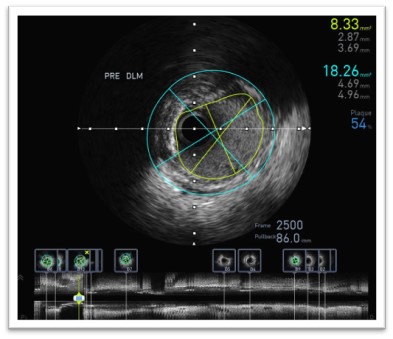
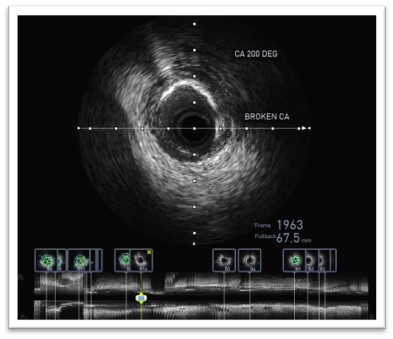
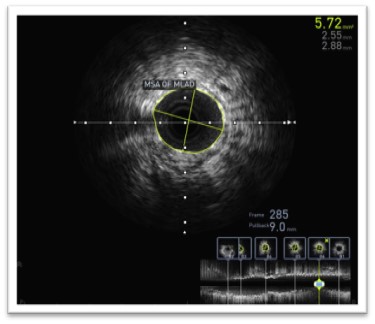
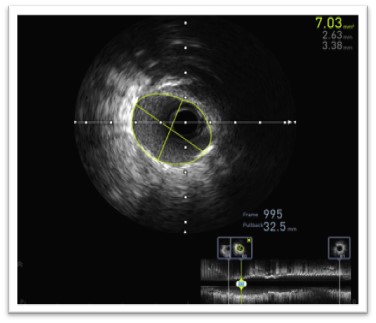
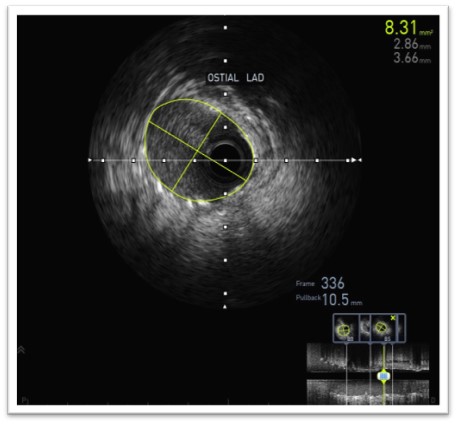
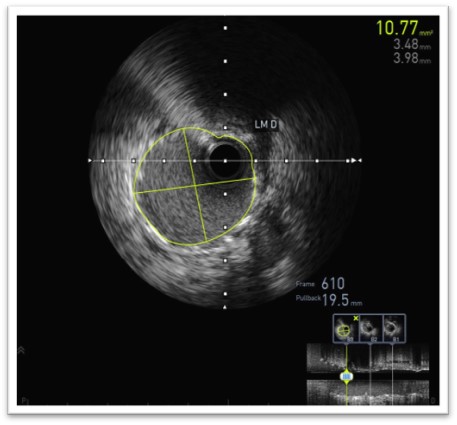
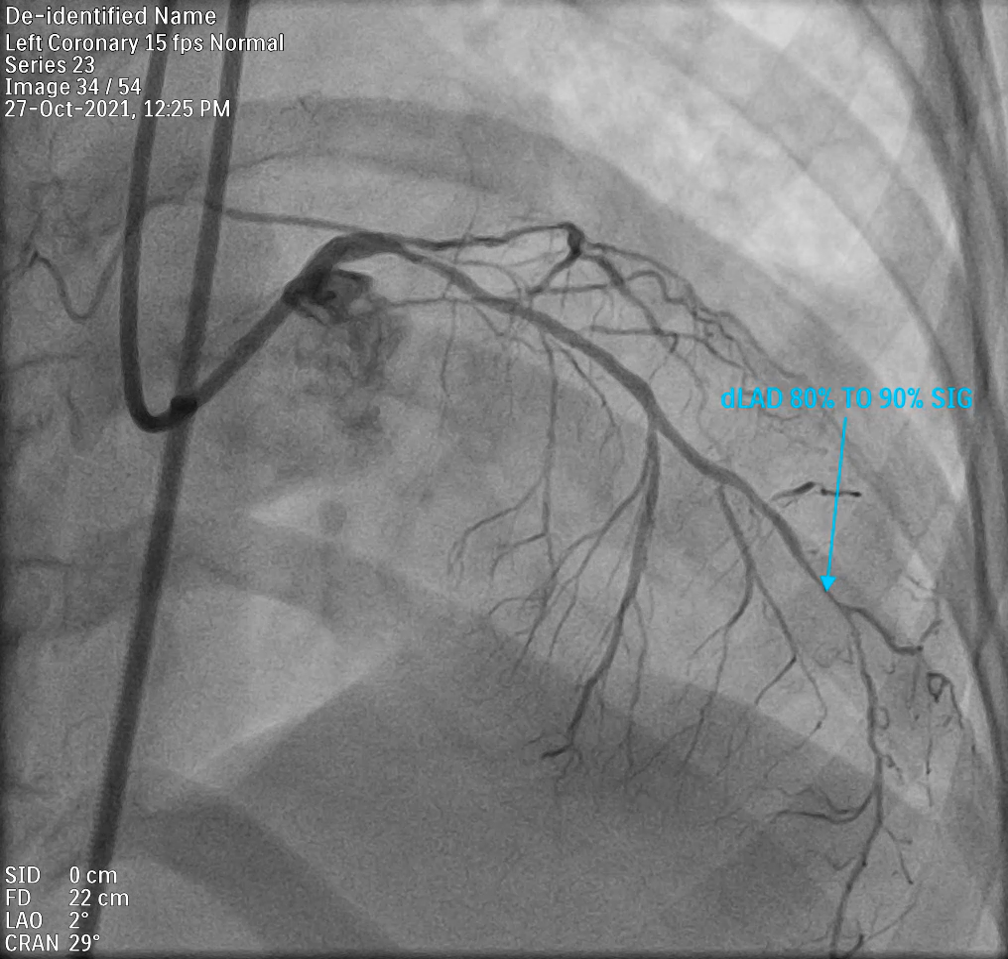
CAG- TVD - Ostio proximal LAD moderately calcified with eccentric 80-90% disease. - Ostioproximal LCX 70-80% lesion. Before bifurcating into OM3 & LPL1 circumflex has 80-90% disease. - RCA proximal - 60-70% lesion. dRCA- 50-60% lesion. PDA & PLB have diffuse disease.CATH STUDY- Pulmonary artery pressure- 72/32 mmHg- RA Pressure- 20 mmHgSYNTAX SCORE- 30
Media29.mp4
Media30.mp4
Media31.mp4
Media32.mp4
Interventional Management
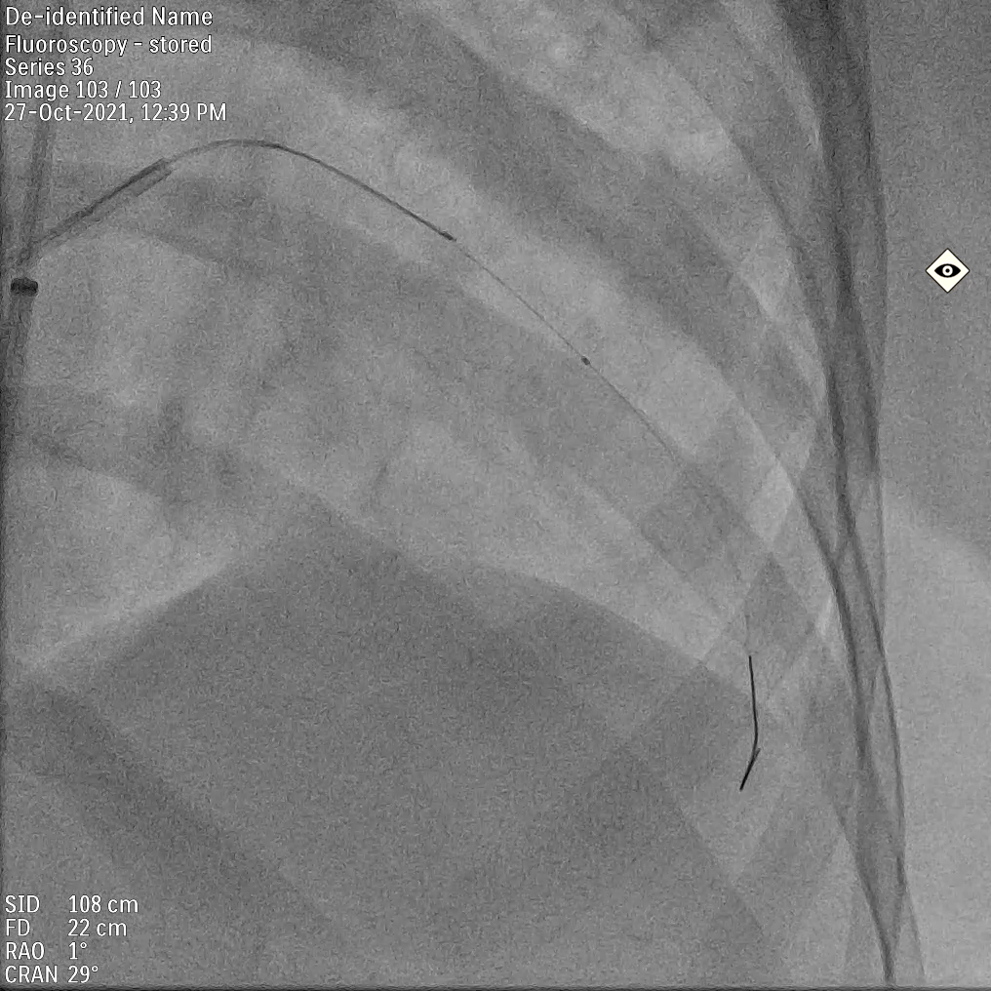
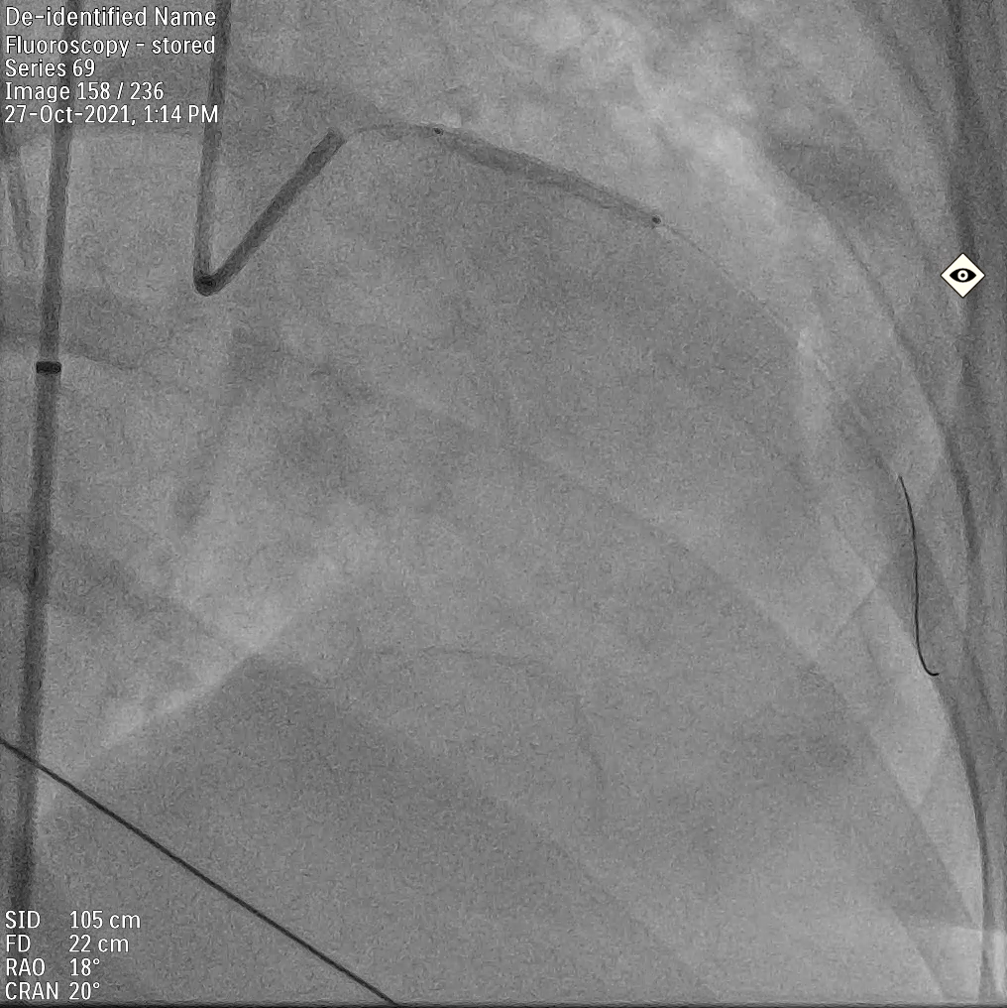
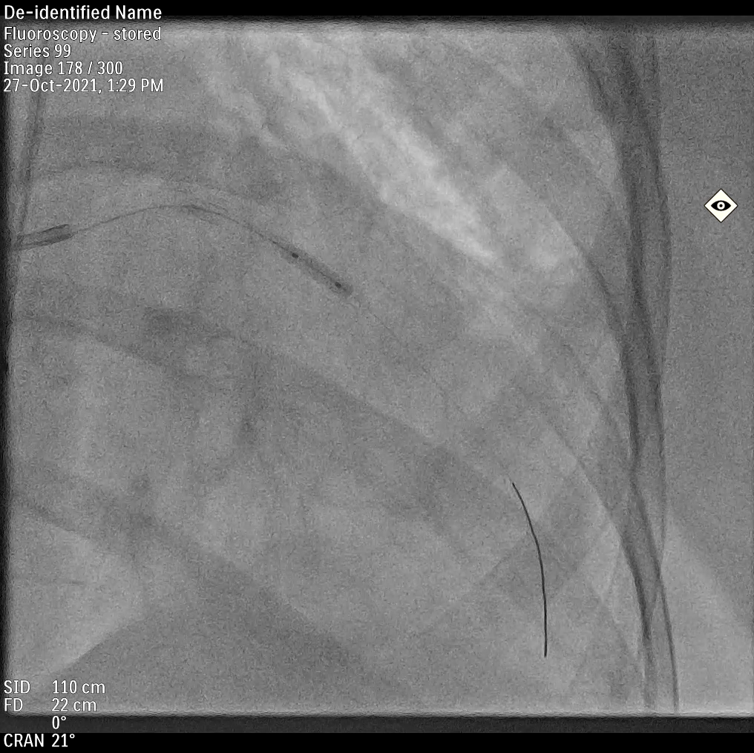
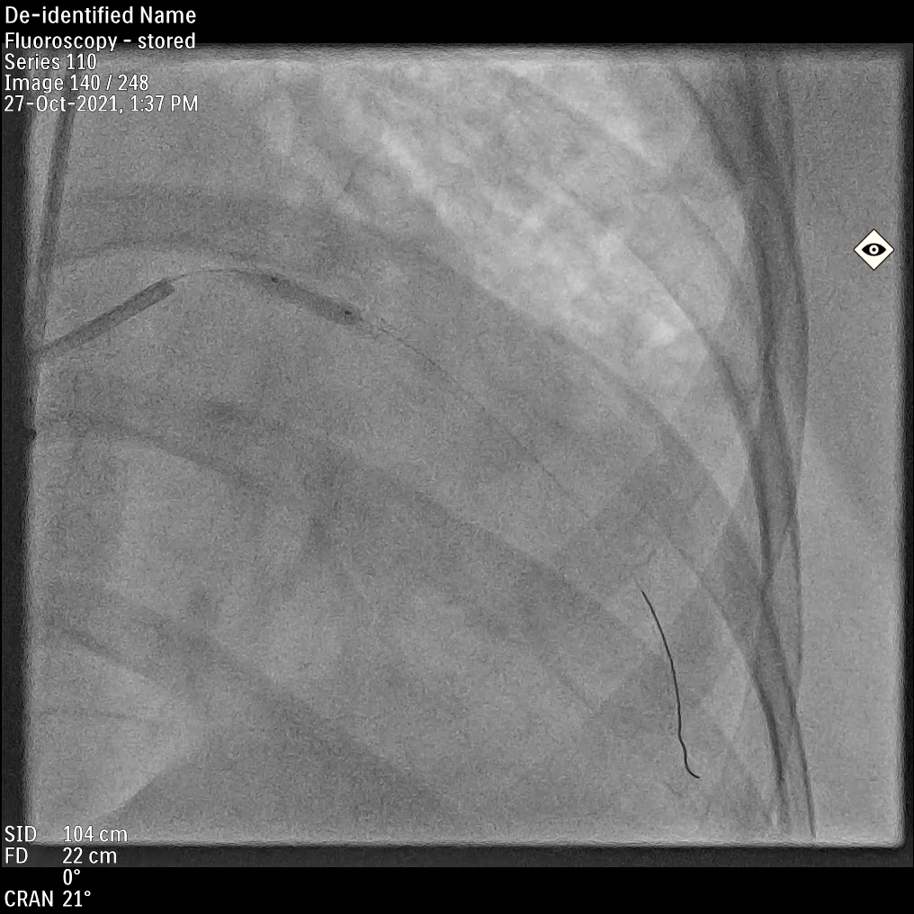
Procedural Step
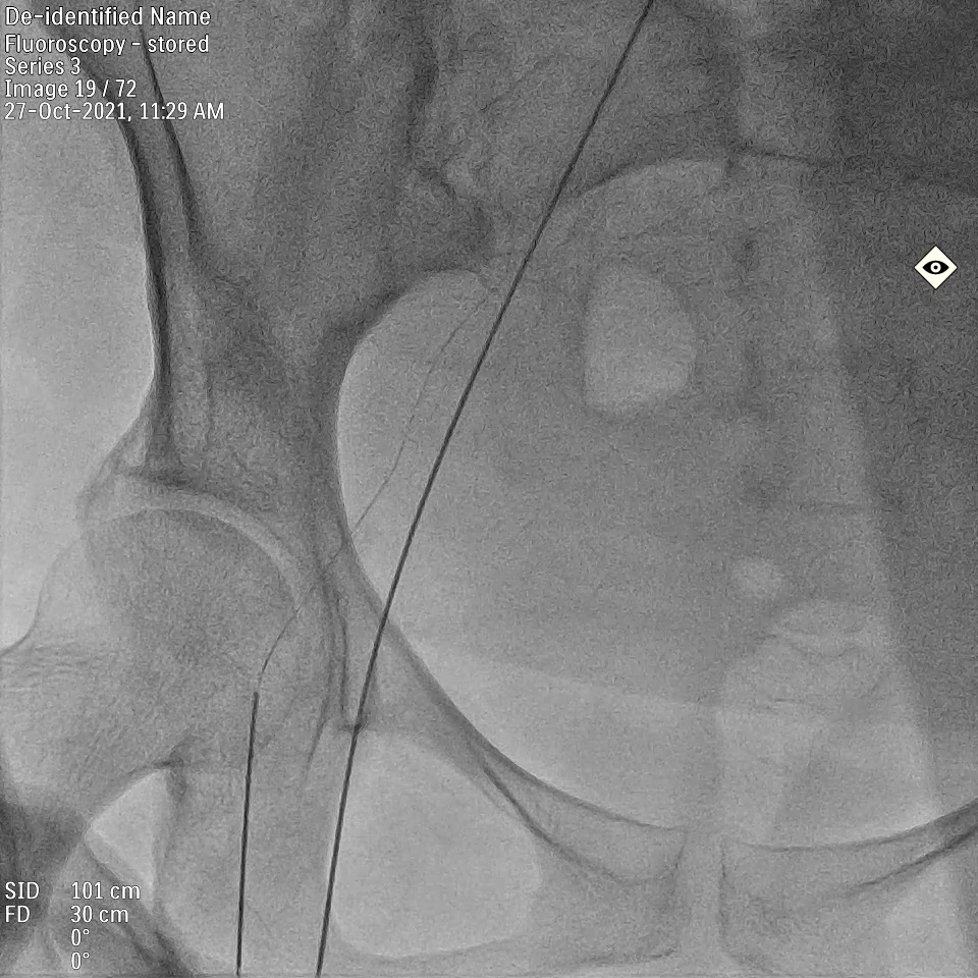
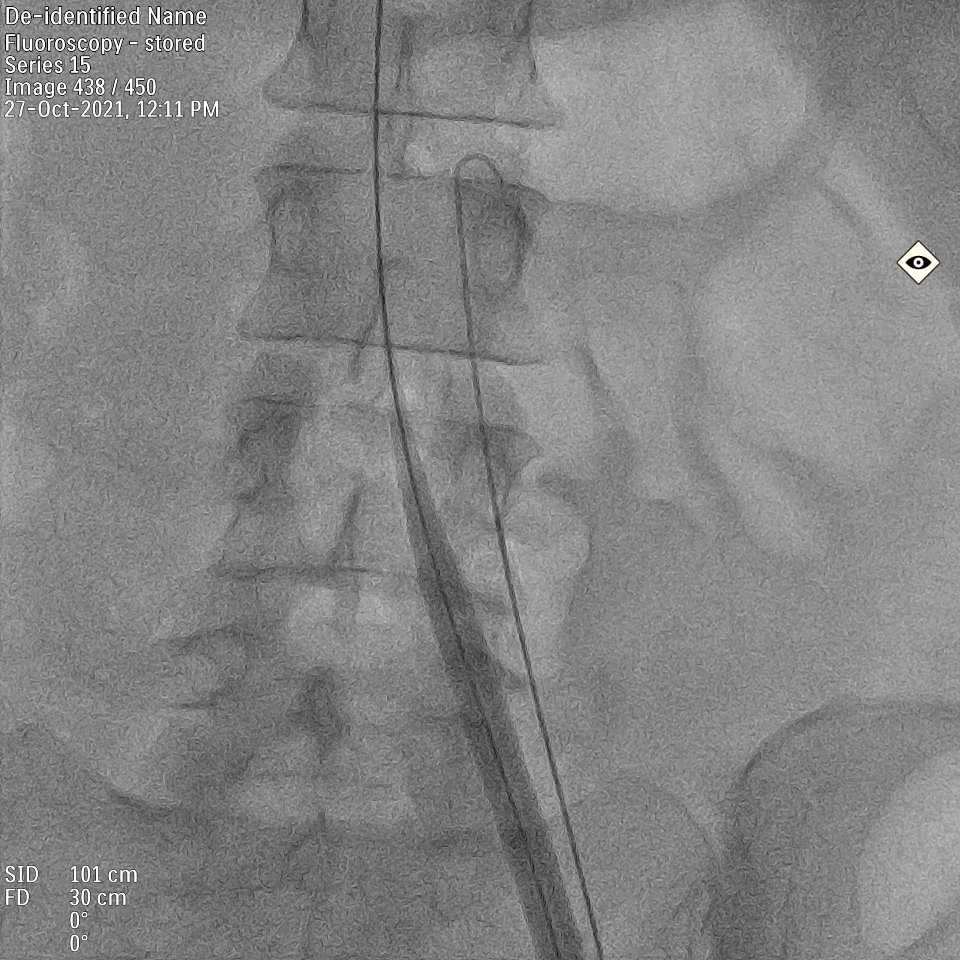
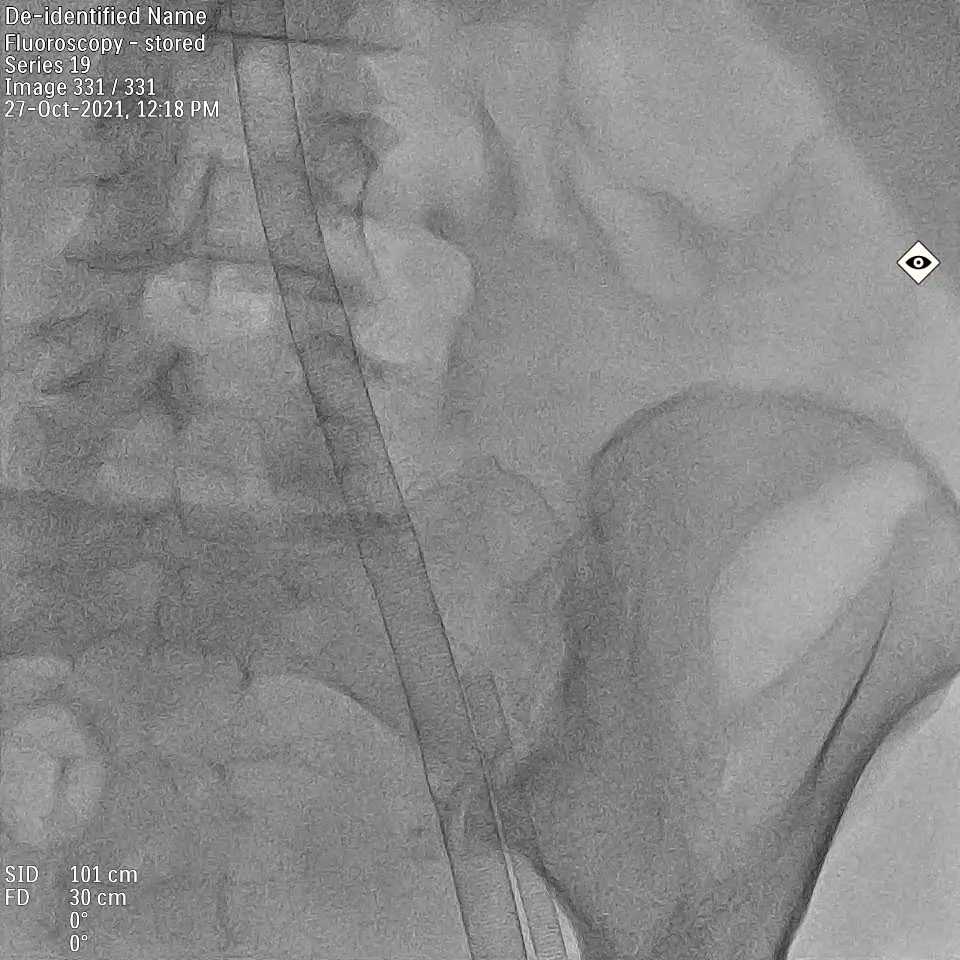
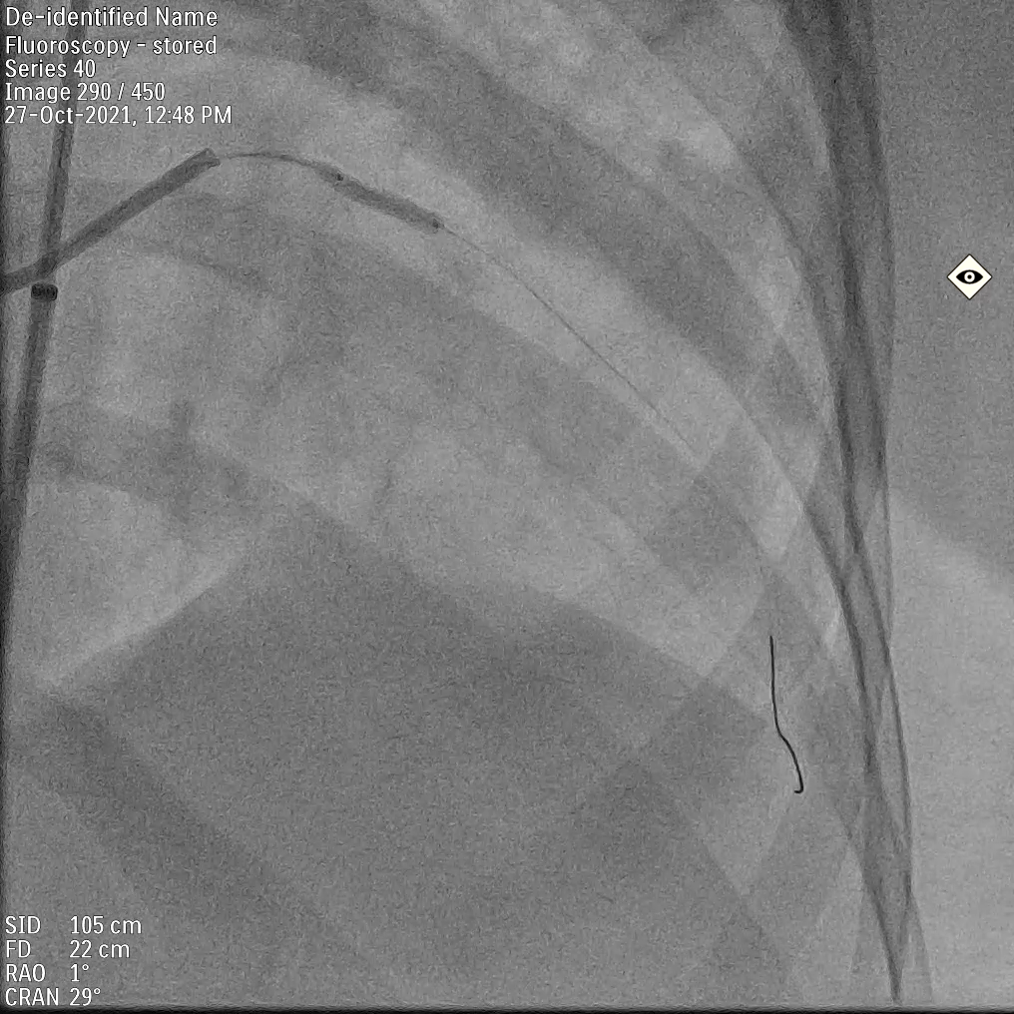
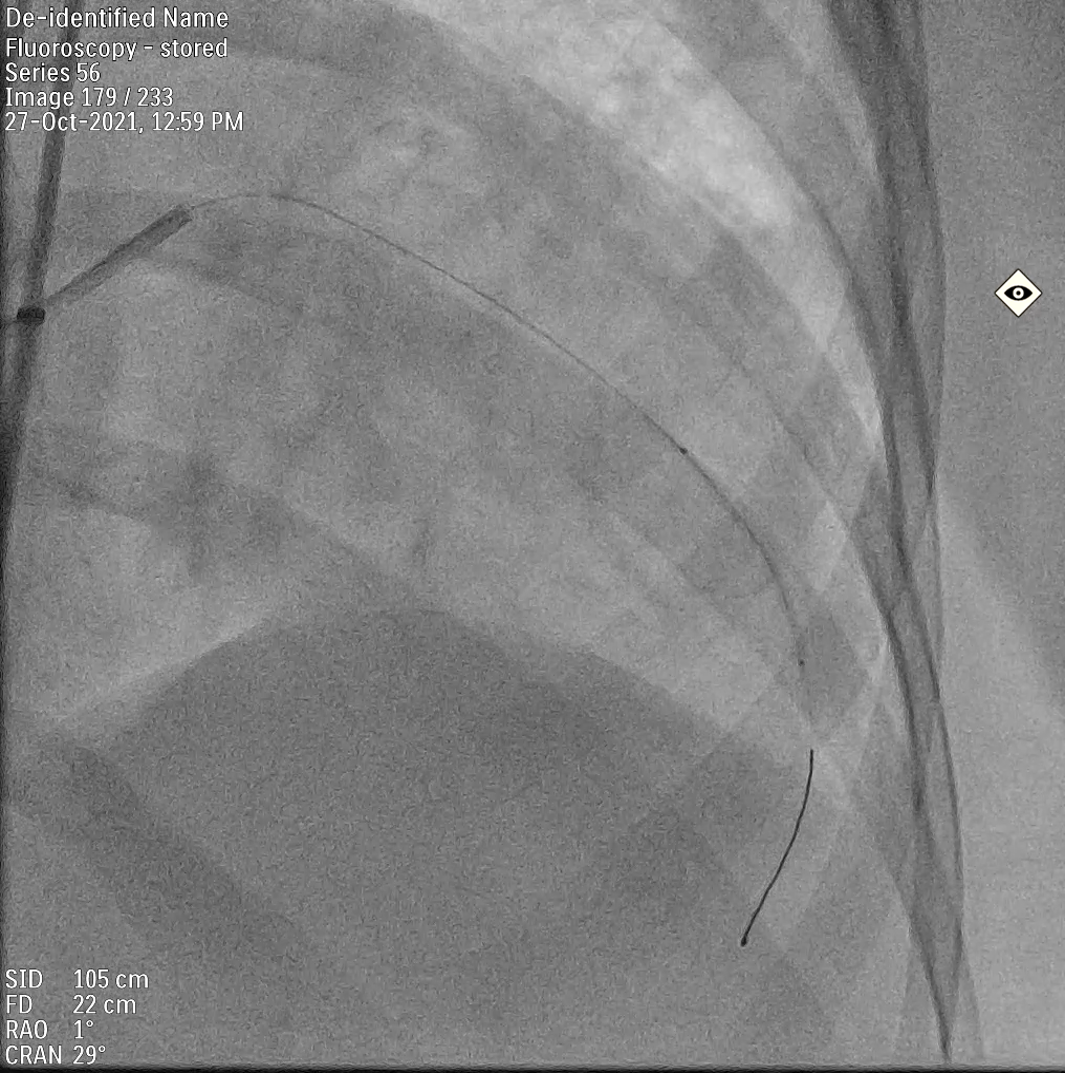
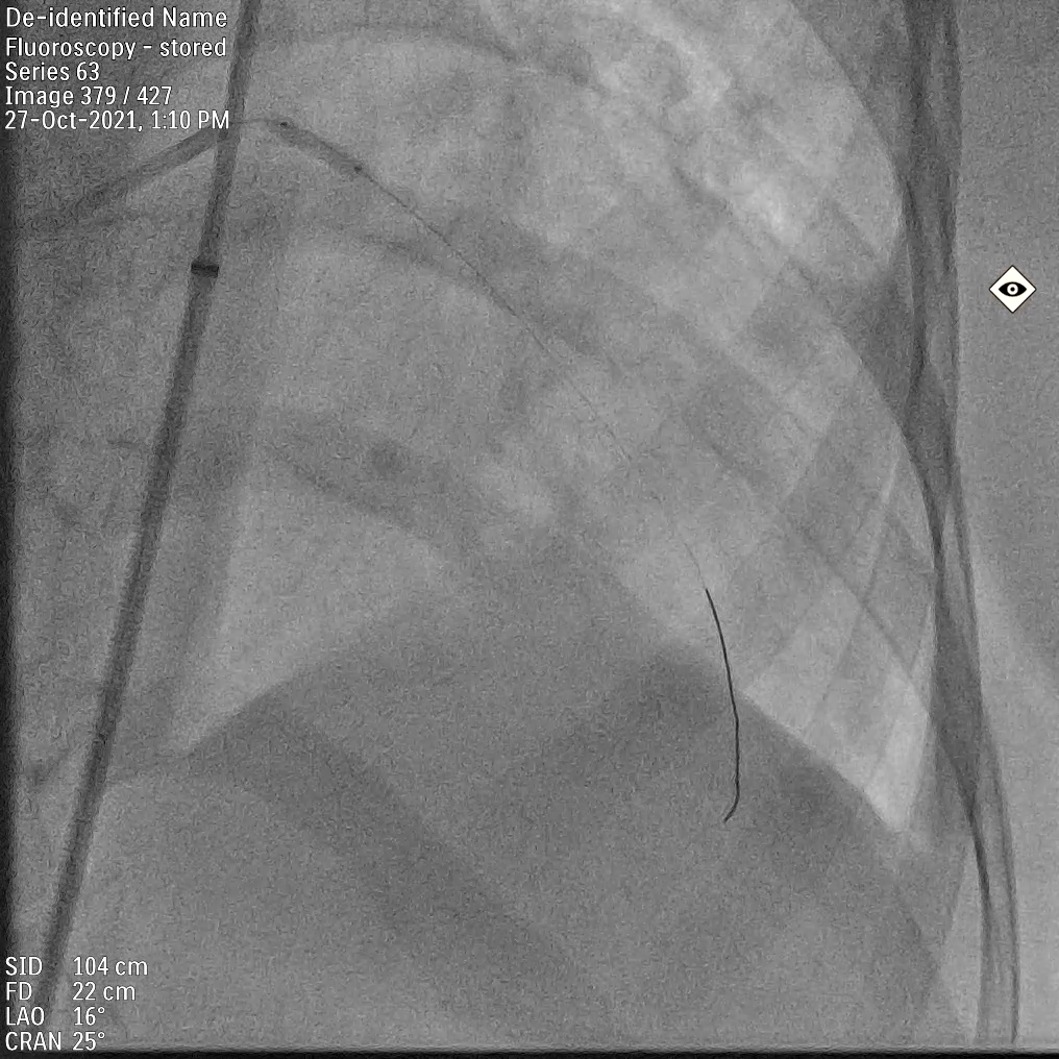
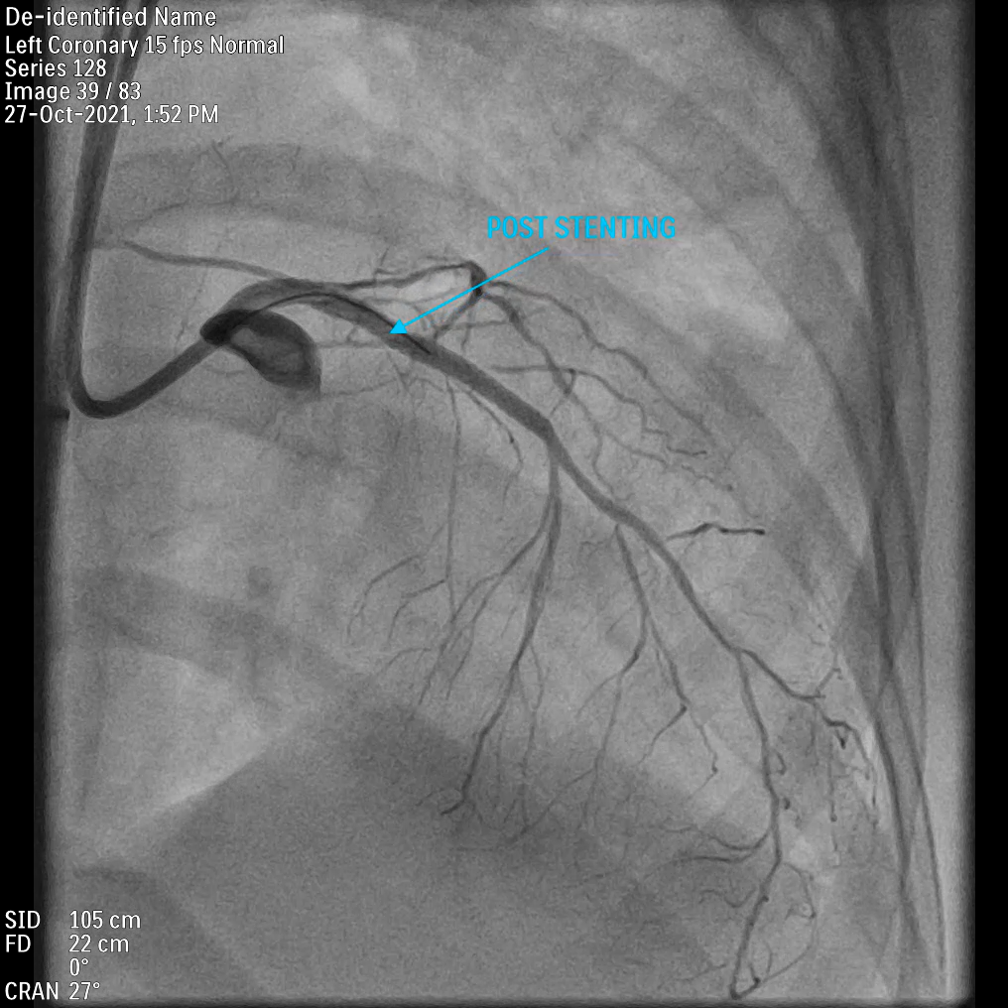
Rt. femoral artery access secured with 8F sheath.Lt. femoral artery (FA) access secured with 15 F ECMO cannula and Lt. Femoral vein with 25 F ECMO cannula.




Case Summary
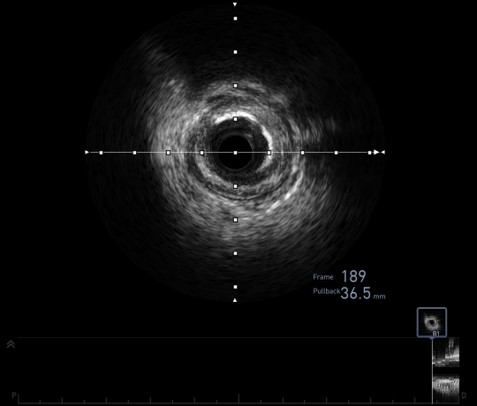
- Even in patients who are declined for CABG, identifying the anatomy, accessing the viability, and revascularizing them with the help of mechanical circulatory device helps.- Viability assessment prevents unnecessary stenting.- Heart team approach plays the important role in CHIP.- Vessel bed preparation is important for success of PCI.- Drug eluting balloon angioplasty shows good result in diffusely diseased vessel.