
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-135
Chronic Stable Lesion Causing Acute Mesentric Ischemia: Mere Mystery Without IVUS
By Ashwani Sharma
Presenter
Ashwani Sharma
Authors
Ashwani Sharma1
Affiliation
Fortis Escorts Hospital, India1,
View Study Report
TCTAP C-135
ENDOVASCULAR - Complications
Chronic Stable Lesion Causing Acute Mesentric Ischemia: Mere Mystery Without IVUS
Ashwani Sharma1
Fortis Escorts Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Mr. D P
Relevant Clinical History and Physical Exam
He has been suffering from abdominal pain for 5 days. There was no clinical localization. Similar pain had occurred 9 months ago which was managed symptomatically with OTC drugs without detailed investigations. He was a smoker. There was no history of other risk factors.
Relevant Test Results Prior to Catheterization
He came to our center on Nov 19th. The abdominal pain was reduced and flatus was being passed. Abdomen was tense. Bowel sounds were sluggish. All other systemic examination was unremarkable.
S. Lactate level was normal. UGI endoscopy was normal.
CECT abdomen revealed ostio proximal thrombotic lesion in SMA.

S. Lactate level was normal. UGI endoscopy was normal.
CECT abdomen revealed ostio proximal thrombotic lesion in SMA.
Relevant Catheterization Findings
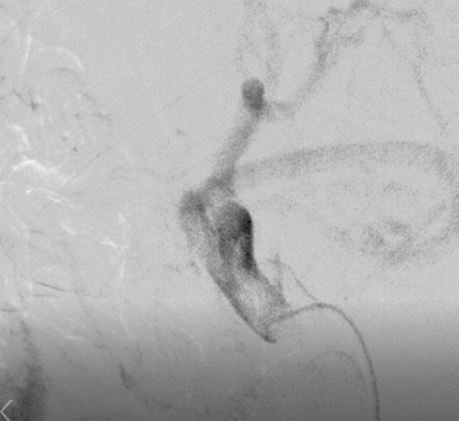
Coronary angiography was normal. Coeliac trunk was normal. There was plaque in ostio proximal SMA which looked stable. IMA branches were arising from SMA.

Interventional Management
Procedural Step
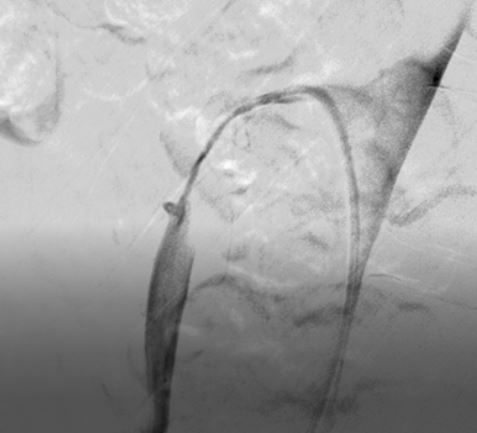
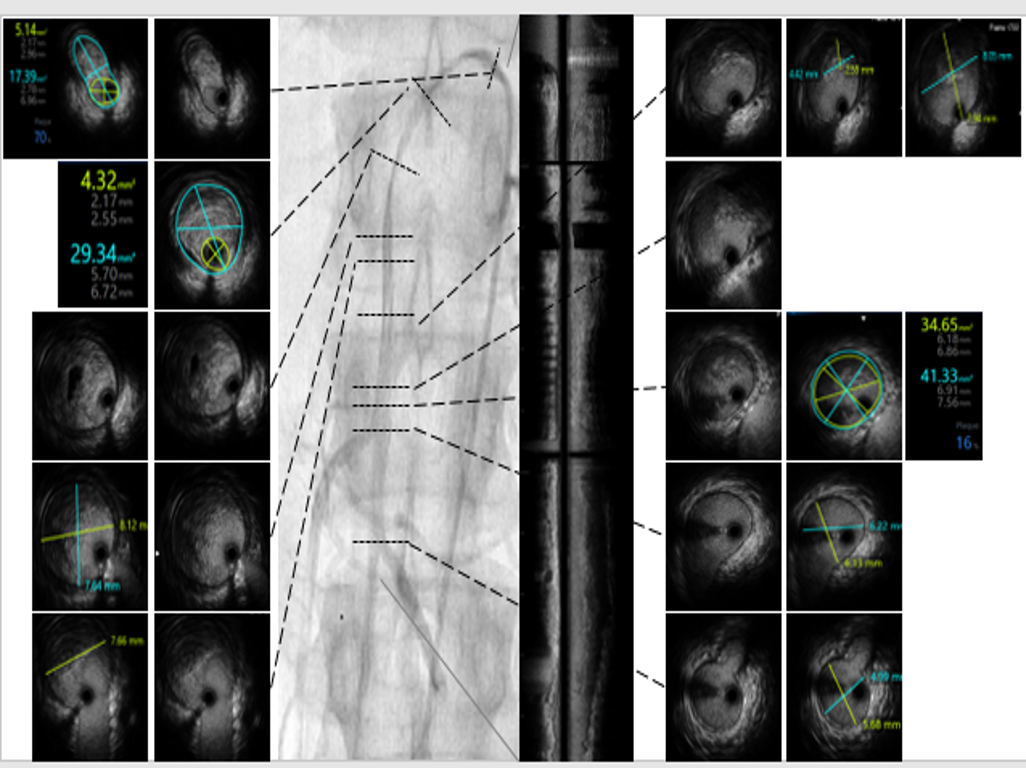
Being a stable lesion, acute presentation was unexplained so IVUS was performed. It revealed ostio-proximal plaque for a length of 38 mm. It was ulcerated at its distal end with superimposed thrombus which was freely hanging in the lumen distally for a length of around 40 mm. It was thought that thrombo-suction alone will not help due to tight proximal segment. If dilatation followed by stent is planned, then there will be unavoidable distal embolization. To reduce the thrombus burden as well as to prevent distal migration, 5 F multihole MPA catheter was advanced and Streptokinase infusion was started at 5 pm. During this maneuver there was abdominal pain which was worsening. Patient was not responding to repeated opioid analgesics with tense abdomen. At 7 pm, it was decided that possibly there was distal embolization or compromise in the flow due to MPA catheter: in both situations, proximal lesion should be fixed. So SES 8 x 80 mm was deployed in ostio proximal SMA; however, there was geographical miss at ostium. He was now pain free. So after post dilatation another BES (for precise ostial placement) was advanced. It was not crossing the proximal part of the stent & degloving occurred in manipulation to advance. It was snares out and another 7 x 17 mm BES was deployed and post dilated with 8 mm balloon successfully. During removal the balloon broke and en mass removal was done. Accidentally 9F sheath also came out. Manual compression was performed till hemostasis.
 37 GEOGRAPHICAL MISS.avi
37 GEOGRAPHICAL MISS.avi
54 DRAWN IN LONG SHEATH 8 F SHEATH.avi
Case Summary
Diagnosis of acute mesenteric ischemia is usually delayed.
Intra-vascular imaging helped to decipher the enigma of acute presentation by stable/chronic lesion.
Patience along with well-equipped catheterization labs are the cornerstone in successfully handling the nightmares.