
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-129
Endovascular Management of Complicated IgG4-Related Disease Periaortitis Refractory to Medical Therapy
By Mohieldin Hezima, Yogesh Acharya, Joshua Ramjohn, David Miresse, Omer Omer, Hesham Elzomor, Osama Soliman, Sherif Sultan
Presenter
Mohieldin Hezima
Authors
Mohieldin Hezima1, Yogesh Acharya1, Joshua Ramjohn1, David Miresse1, Omer Omer1, Hesham Elzomor2, Osama Soliman2, Sherif Sultan1
Affiliation
Western Vascular Institute, University Hospital Galway, Ireland1, National University of Ireland, Galway, Ireland2,
View Study Report
TCTAP C-129
ENDOVASCULAR - Aorta Disease and Intervention
Endovascular Management of Complicated IgG4-Related Disease Periaortitis Refractory to Medical Therapy
Mohieldin Hezima1, Yogesh Acharya1, Joshua Ramjohn1, David Miresse1, Omer Omer1, Hesham Elzomor2, Osama Soliman2, Sherif Sultan1
Western Vascular Institute, University Hospital Galway, Ireland1, National University of Ireland, Galway, Ireland2,
Clinical Information
Patient initials or Identifier Number
P.E
Relevant Clinical History and Physical Exam
A 70-year-old gentleman with NIDDM, HTN and hypothyroidism who have been on glucocorticoid therapy since 2015 for IgG4-RelatedDisease (IgG4-RD) with a good initial response to treatment. He had CT-guided left para-aortic core biopsy that was complicated by massive bleeding managed by coil embolization. Histopathology showed characteristic features of IgG4-RD. In 2017, the patient was referred to our vascular clinic with incidental findings of soft tissue thickening around the mid-distal.
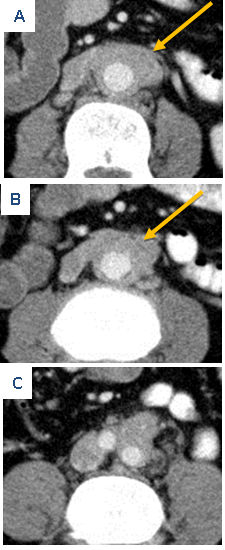
Relevant Test Results Prior to Catheterization
infrarenal aorta extending to both common iliac arteries on his last routine CT follow up scans (Fig.1 A, B, C, yellow arrow; video 1: axial movie CT aortogram). He had chronic abdominal and back pain with recurrent UTI for four years, however, there was no evidence of urinary tract obstruction and physical examination was unremarkable. We planned to continue medical treatment with follow-up.
 Video 1.mp4
Video 1.mp4
Relevant Catheterization Findings
Eight months later he had a relapse and developed hydronephrosis. Right nephrostomy and antegrade JJ-stent was inserted following a complicated failed retrograde approach. In addition, rituximab was started to control his relapse. He continues to deteriorate with multiple relapses and worsening abdominal and back pain unresponsive to opiates. Therefore, azathioprine was initiated, however, recurrent pain was significantly affecting his quality of life.
Video 2.mp4
Video 3.mp4
Interventional Management
Procedural Step
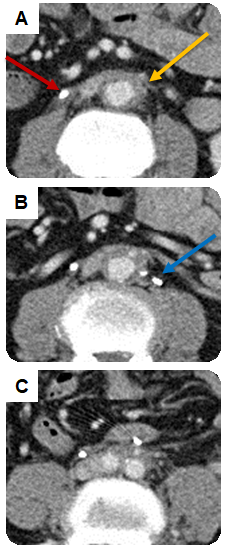
After frequent relapses despite optimum medical therapy, a decision was made to proceed with endovascular treatment. PreoperativeCT angiogram showed persistent soft tissue thickening (Fig. 2A, B, C, yellow arrow; video 2: axial movie CT aortogram), right JJ-stent in place (Fig. 2A, red arrow) and previous embolization coil (Fig. 2B, blue arrow).
Video 4.mp4
Video 5.mp4
Case Summary
To our knowledge, this is the 2nd successful case in literature to treat IgG4-RD periaortitis not associated with inflammatory aneurysm with endovascular stent graft after refractory medical therapy. Further studies are needed to investigate the long-term outcome of the endovascular approach in such a rare disease entity.